

Effects of total fat intake on bodyweight in children
- PMID: 29446437
- PMCID: PMC6491333
- DOI: 10.1002/14651858.CD012960
Effects of total fat intake on bodyweight in children
Update in
-
Effects of total fat intake on bodyweight in children.Cochrane Database Syst Rev. 2018 Jul 5;7(7):CD012960. doi: 10.1002/14651858.CD012960.pub2. Cochrane Database Syst Rev. 2018. PMID: 29974953 Free PMC article.
Abstract
Background: As part of efforts to prevent childhood overweight and obesity, we need to understand the relationship between total fat intake and body fatness in generally healthy children.
Objectives: To assess the effects of total fat intake on measures of weight and body fatness in children and young people not aiming to lose weight.
Search methods: For this update we revised the previous search strategy and ran it over all years in the Cochrane Library, MEDLINE (Ovid), MEDLINE (PubMed), and Embase (Ovid) (current to 23 May 2017). No language and publication status limits were applied. We searched the World Health Organization International Clinical Trials Registry Platform and ClinicalTrials.gov for ongoing and unpublished studies (5 June 2017).
Selection criteria: We included randomised controlled trials (RCTs) in children aged 24 months to 18 years, with or without risk factors for cardiovascular disease, randomised to a lower fat (30% or less of total energy (TE)) versus usual or moderate-fat diet (greater than 30%TE), without the intention to reduce weight, and assessed a measure of weight or body fatness after at least six months. We included prospective analytical cohort studies in these children if they related baseline total fat intake to weight or body fatness at least 12 months later. We duplicated inclusion decisions and resolved disagreement by discussion with other authors.
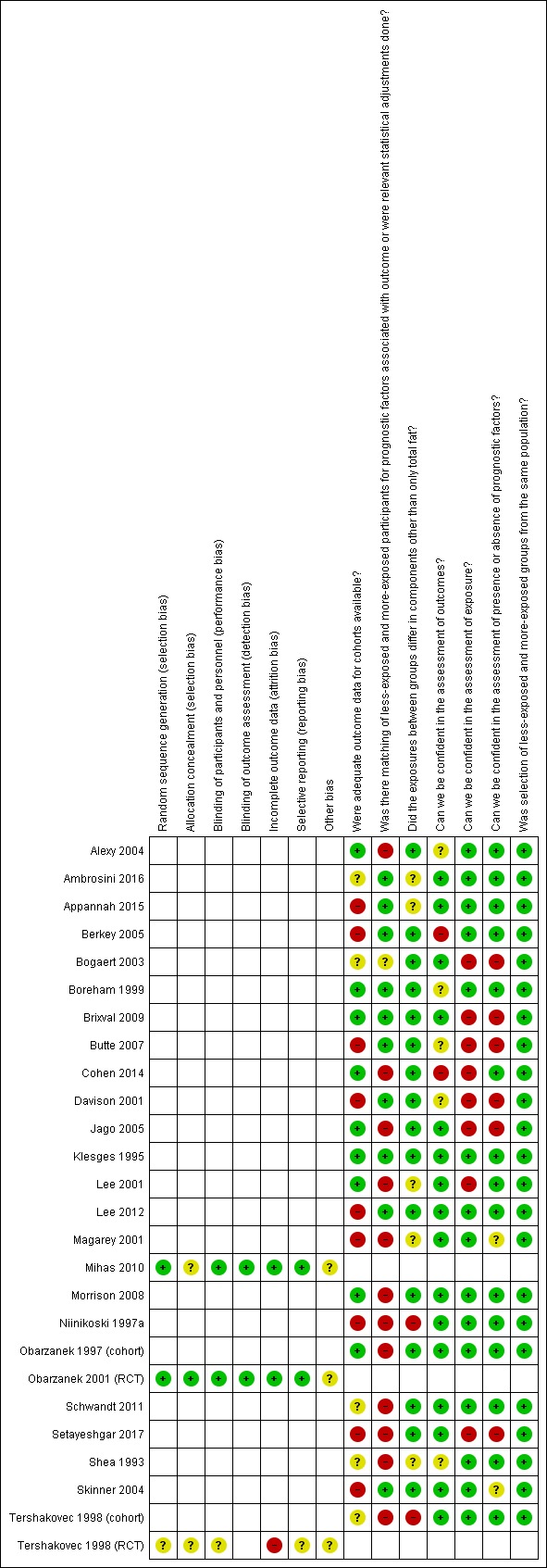
Data collection and analysis: We extracted data on participants, interventions or exposures, controls and outcomes, and trial or cohort quality characteristics, as well as data on potential effect modifiers, and assessed risk of bias for all included studies. We extracted outcome data using the following time point ranges, when available: RCTs: baseline to six months, six to 12 months, one to two years, two to five years and more than five years; cohort studies: baseline to one year, one to two years, two to five years, five to 10 years and more than 10 years. We planned to perform random-effects meta-analyses with relevant subgrouping, and sensitivity and funnel plot analyses where data allowed.
Main results: We included 24 studies comprising three parallel-group RCTs (n = 1054 randomised) and 21 prospective analytical cohort studies (about 25,059 children completed). Twenty-three were conducted in high-income countries. No meta-analyses were possible, since only one RCT reported the same outcome at each time point range for all outcomes, and cohort studies were too heterogeneous.For the RCTs, concerns about imprecision and poor reporting limited our confidence in our findings. In addition, the inclusion of hypercholesteraemic children in two trials raised concerns about applicability. Lower versus usual or modified total fat intake may have made little or no difference to weight over a six- to twelve month period (mean difference (MD) -0.50 kg, 95% confidence interval (CI) -1.78 to 0.78; 1 RCT; n = 620; low-quality evidence), nor a two- to five-year period (MD -0.60 kg, 95% CI -2.39 to 1.19; 1 RCT; n = 612; low-quality evidence). Compared to controls, lower total fat intake (30% or less TE) probably decreased BMI in children over a one- to two-year period (MD -1.5 kg/m2, 95% CI -2.45 to -0.55; 1 RCT; n = 191; moderate-quality evidence), with no other differences evident across the other time points (two to five years: MD 0.00 kg/m2, 95% CI -0.63 to 0.63; 1 RCT; n = 541; greater than five years; MD -0.10 kg/m2, 95% CI -0.75 to 0.55; 1 RCT; n = 576; low-quality evidence). Lower fat intake probably slightly reduced total cholesterol over six to 12 months compared to controls (MD -0.15 mmol/L, 95% CI -0.24 to -0.06; 1 RCT; n = 618; moderate-quality evidence), but may make little or no difference over longer time periods. Lower fat intake probably slightly decreased low-density lipoprotein (LDL) cholesterol over six to 12 months (MD -0.12 mmol/L, 95% CI -0.20 to -0.04; 1 RCT; n = 618, moderate-quality evidence) and over two to five years (MD -0.09, 95% CI -0.17 to -0.01; 1 RCT; n = 623; moderate-quality evidence), compared to controls. However, lower total fat intake probably made little or no difference to HDL-C over a six- to 12-month period (MD -0.03 mmol/L, 95% CI -0.08 to 0.02; 1 RCT; n = 618; moderate-quality evidence), nor a two- to five-year period (MD -0.01 mmol/L, 95% CI -0.06 to 0.04; 1 RCT; n = 522; moderate-quality evidence). Likewise, lower total fat intake probably made little or no difference to triglycerides in children over a six- to 12-month period (MD -0.01 mmol/L, 95% CI -0.08 to 0.06; 1 RCT; n = 618; moderate-quality evidence). Lower versus usual or modified fat intake may make little or no difference to height over more than five years (MD -0.60 cm, 95% CI -2.06 to 0.86; 1 RCT; n = 577; low-quality evidence).Over half the cohort analyses that reported on primary outcomes suggested that as total fat intake increases, body fatness measures may move in the same direction. However, heterogeneous methods and reporting across cohort studies, and predominantly very low-quality evidence, made it difficult to draw firm conclusions and true relationships may be substantially different.
Authors' conclusions: We were unable to reach firm conclusions. Limited evidence from three trials that randomised children to a lower total fat intake (30% or less TE) versus usual or modified fat intake, but with no intention to reduce weight, showed small reductions in body mass index, total- and LDL-cholesterol at some time points with lower fat intake compared to controls, and no consistent differences in effects on weight, high-density lipoprotein (HDL) cholesterol or height. Associations in cohort studies that related total fat intake to later measures of body fatness in children were inconsistent and the quality of this evidence was mostly very low. Twenty-three out of 24 included studies were conducted in high-income countries, and may not be applicable in low- and middle-income settings. High-quality, longer-term studies are needed, that include low- and middle-income settings and look at both possible benefits and risks.
Conflict of interest statement
The World Health Organization (WHO) provided funding to Stellenbosch University towards the cost of carrying out the update of this systematic review. CN, MV, SD and AS are partly supported by the Effective Health Care Research Consortium. This Consortium is funded by UK aid from the UK Government for the benefit of developing countries (Grant: 5242). The views expressed in this publication do not necessarily reflect UK government policy.
Figures



















References
References to studies included in this review
-
- Alexy U, Schultze‐Pawlitschko V, Sichert‐Hellert W, Kersting M. Cluster analysis of individuals with similar trends of fat intake during childhood and adolescence: a new approach to analyzing dietary data. Nutrition Research 2005;25:251‐60.
- Alexy U, Sichert‐Hellert W, Kersting M, Schultze‐Pawlitschko V. Pattern of long‐term fat intake and BMI during childhood and adolescence‐results of the DONALD Study. International Journal of Obesity Related Metabolic Disorders 2004;28(10):1203‐9. [DOI: 10.1038/sj.ijo.0802708] - DOI - PubMed
-
- Ambrosini G, Johns D, Northstone K, Emmett PM, Jebb SA. Free sugars and total fat are important characteristics of a dietary pattern associated with adiposity across childhood and adolescence. Journal of Nutrition 2016;146(4):778‐84. - PMC - PubMed
- Ambrosini G, Johns D, Northstone K, Jebb S. Fat, sugar or both? A prospective analysis of dietary patterns and adiposity in children. FASEB Journal 2015;29:1.
- Ambrosini GL, Emmett, PM, Northstone K, Howe LD, Tilling K, Jebb SA. Identification of a dietary pattern prospectively associated with increased adiposity during childhood and adolescence. International Journal of Obesity (2005) 2012;36(10):1299‐305. - PMC - PubMed
- Golding J, Pembrey M, Jones R, ALSPAC Study Team. ALSPAC‐The Avon Longitudinal Study of Parents and Children. I. Study methodology. Paediatric and Perinatal Epidemiology 2001;15:74‐87. - PubMed
- Johnson L, Mander AP, Jones LR, Emmett PM, Jebb SA. A prospective analysis of dietary energy density at age 5 and 7 years and fatness at 9 years among UK children. International Journal of Obesity (2005) 2008;32(4):586‐93. - PubMed
- Johnson L, Mander AP, Jones LR, Emmett PM, Jebb SA. Energy‐dense, low‐fiber, high‐fat dietary pattern is associated with increased fatness in childhood. American Journal of Clinical Nutrition 2008;87(4):846‐54. - PubMed
- Rogers IS, Emmett PM, Alspac Study Team. Fat content of the diet among preschool children in southwest Britain: II. relationship with growth, blood lipids, and iron status. Pediatrics 2001;108(3):E49. - PubMed
-
- Ambrosini GL, Klerk NH, O'Sullivan TA, Beilin LJ, Oddy WH. The reliability of a Food Frequency Questionnaire for use among adolescents. European Journal of Clinical Nutrition 2009;63:1251‐9. - PubMed
- Appannah G, Pot GK, Huang RC, Oddy WH, Beilin LJ, Mori TA, et al. Identification of a dietary pattern associated with greater cardiometabolic risk in adolescence. Nutrition, Metabolism, and Cardiovascular Diseases : NMCD 2015;25(7):643‐50. - PMC - PubMed
-
- Berkey CS, Rockett H, Willett WC, Colditz GA. Milk, dairy fat, dietary calcium, and weight gain: a longitudinal study of adolescents. Archives of Pediatrics and Adolescent Medicine 2005;159(6):543‐50. - PubMed
- Berkey CS, Rockett HR, Field AE, Gillman MW, Frazier AW, Camargo CA Jr, et al. Activity, dietary intake, and weight changes in a longitudinal study of preadolescent and adolescent boys and girls. Pediatrics 2000;105(4):E56. - PubMed
References to studies excluded from this review
-
- Adair LS, Kuzawa CW, Borja J. Maternal energy stores and diet composition during pregnancy program adolescent blood pressure. Circulation 2001;104(9):1034‐9. - PubMed
-
- Agostoni C, Riva E, Scaglioni S, Marangoni F, Radaelli G, Giovannini M. Dietary fats and cholesterol in Italian infants and children. American Journal of Clinical Nutrition 2000;72(5 Suppl):1384S‐91S. - PubMed
-
- Ahola‐Olli AV, Pitkanen N, Kettunen J, Oikonen MK, Mikkila V, Lehtimaki T, et al. Interactions between genetic variants and dietary lipid composition: effects on circulating LDL cholesterol in children. American Journal of Clinical Nutrition 2014;100(6):1569‐77. - PubMed
-
- Alexy U, Sichert‐Hellert W, Kersting M. Fifteen‐year time trends in energy and macronutrient intake in German children and adolescents: results of the DONALD study. British Journal of Nutrition 2002;87(6):595‐604. - PubMed
-
- Altwaijri YA, Day RS, Harrist RB, Dwyer J, Ausman LM, Labarthe DR. Sexual maturation affects diet‐blood total cholesterol association in children: Project HeartBeat!. American Journal of Preventive Medicine 2009;37(1 Suppl):S65‐70. - PubMed
References to studies awaiting assessment
-
- Khalil H, Murrin C, Viljoen K, O'Brien J, Segurado R, Kelleher C. Developmental trajectories of body mass index (BMI) from birth to late childhood and their relation with paternal and child nutrients intake. Obesity Facts 2014;7:145. [DOI: 10.1159/000363668] - DOI
- Khalil H, Murrin C, Viljoen K, Segurado R, Somerville R, O'Brien J, et al. Metabolic syndrome risk in Irish children is associated with maternal diet: prospective findings from the lifeways crossgeneration cohort study 2001‐2014. Atherosclerosis 2015;241(1):e171.
-
- Koppes LJ, Boon N, Nooyens ACJ, Mechelen W, Saris WHM. Macronutrient distribution over a period of 23 years in relation to energy intake and body fatness. British Journal of Nutrition 2009;101(1):108‐15. - PubMed
- Twisk JW, Kemper HC, Mechelen W, Post GB, Lenthe FJ. Body fatness: longitudinal relationship of body mass index and the sum of skinfolds with other risk factors for coronary heart disease. International Journal of Obesity and Related Metabolic Disorders 1998;22(9):915‐22. - PubMed
Additional references
-
- Ajala O, English P, Pinkney J. Systematic review and meta‐analysis of different dietary approaches to the management of type 2 diabetes. American Journal of Clinical Nutrition 2013;97:505‐16. - PubMed
-
- Aljadani H, Patterson A, Sibbritt D, Collins C. The association between diet quality and weight change in adults over time: a systematic review of prospective cohort studies. Diet Quality: An Evidence Based Approach. 2. New York (NY): Springer, 2013:3‐27. [DOI: 10.1007/978-1-4614-7315-2_1] - DOI
-
- Aljadani H, Patterson A, Sibbritt D, Collins CE. Diet quality and weight change in adults over time: a systematic review of cohort studies. Current Nutrition Reports 2015;4:88‐101.
-
- Ambrosini GL. Childhood dietary patterns and later obesity: a review of the evidence. Proceedings of the Nutrition Society 2014;73:137‐46. - PubMed
References to other published versions of this review
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous