

Aggressive fluid accumulation is associated with acute kidney injury and mortality in a cohort of patients with severe pneumonia caused by influenza A H1N1 virus
- PMID: 29447205
- PMCID: PMC5813941
- DOI: 10.1371/journal.pone.0192592
Aggressive fluid accumulation is associated with acute kidney injury and mortality in a cohort of patients with severe pneumonia caused by influenza A H1N1 virus
Abstract
Introduction: Fluid accumulation is associated with adverse outcomes such as acute kidney injury (AKI) in critically ill patients. This study aimed to describe the factors associated with AKI in individuals with influenza A H1N1 severe pneumonia, and explore the relation of fluid accumulation with AKI and mortality.
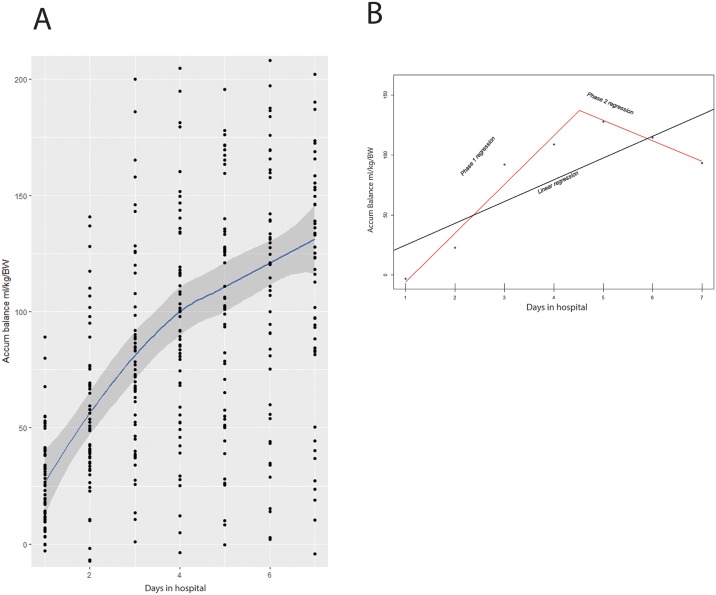
Material and methods: We reviewed medical records of individuals with influenza A H1N1 severe pneumonia and no history of chronic kidney disease, attending a national referral center for respiratory diseases between November 2014 and May 2015. Demographic information, risk factors for AKI, physiologic and laboratory data, outcomes and information on fluid intake and output were recorded. Categorical variables were compared using the chi-square test. Quantitative variables were compared using the Mann-Whitney test. Factors associated with AKI and mortality were identified by binary logistic regression. Linear models of fluid accumulation rates for individuals and groups were estimated using segmented linear regression.
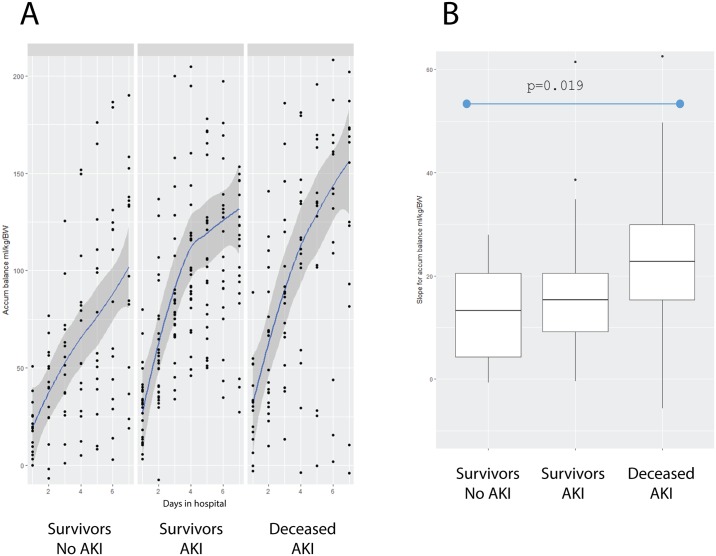
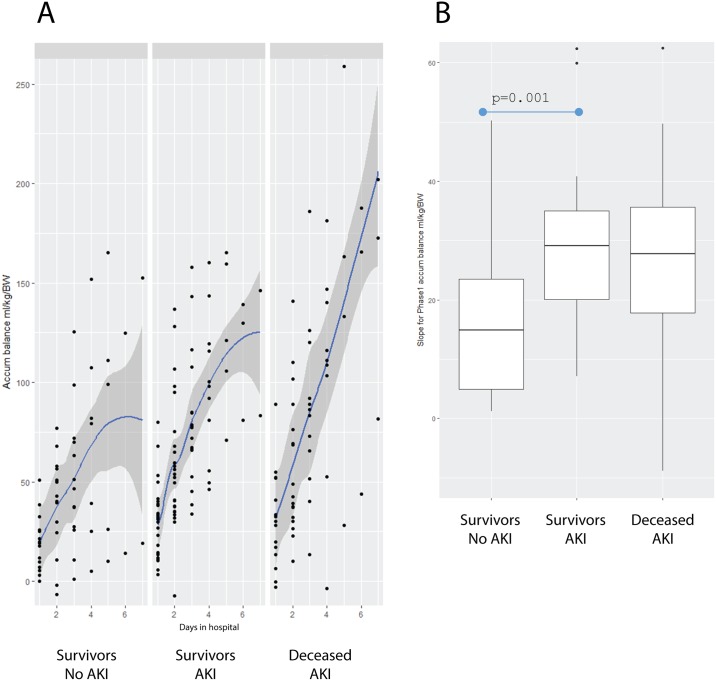
Results: Of 60 patients studied, 43 developed AKI (71.6%). Male gender was protective for AKI (p = 0.019). AKI was associated with nephrotoxic drugs (p = 0.016); PEEP>10 cm H2O on admission (p = 0.031); mortality (p = 0.037); and fluid accumulation ≥10% (fluid overload) at day 7 of hospitalization (p = 0.00026). Mortality was associated with older age (p = 0.009); nephrotoxic drugs (p = 0.034); and higher Pneumonia Severity Index score (112 vs. 76, p = 0.008) on admission. The Deceased-AKI group had a higher rate of fluid accumulation (expressed as ml/kg/body weight) than the Survivors-No AKI group during the study period of 7 days (Survivors-No AKI = 13.31 vs. Deceased-AKI = 22.76, p = 0.019). During the highest phase of fluid accumulation, the Survivors-No AKI group had a slower rate of fluid accumulation than the Survivors-AKI group (14.91 vs. 28.49, p = 0.001).
Conclusions: A high rate of fluid accumulation was associated with AKI and mortality. We support the approach of resuscitation in acute illness, with an early transition to neutral and then negative fluid balances.
Conflict of interest statement
Figures
References
-
- Wald R, Quinn RR, Luo J, Li P, Scales DC, Mamdani MM, et al. Chronic dialysis and death among survivors of acute kidney injury requiring dialysis. JAMA. 2009; 302:1179–1185. doi: 10.1001/jama.2009.1322 - DOI - PubMed
-
- Coca SG, Yusuf B, Shlipak MG, Garg AX, Parikh CR. Long-term risk of mortality and other adverse outcomes after acute kidney injury: a systematic review and metaanalysis. Am J Kidney Dis. 2009; 53: 961–973. doi: 10.1053/j.ajkd.2008.11.034 - DOI - PMC - PubMed
-
- Dennen P, Douglas IS, Anderson R. Acute kidney injury in the intensive care unit: an update and primer for the intensivist. Crit Care Med. 2010; (38): 261–75. doi: 10.1097/CCM.0b013e3181bfb0b5 - DOI - PubMed
-
- Prowle JR, Echeverri JE, Ligabo EV, Ronco C, Bellomo R. Fluid balance and acute kidney injury. Nat Rev Nephrol. 2010; 6:107–15. doi: 10.1038/nrneph.2009.213 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
