

Differences between fellow eyes of acute and chronic primary angle closure (glaucoma): An ultrasound biomicroscopy quantitative study
- PMID: 29447247
- PMCID: PMC5814014
- DOI: 10.1371/journal.pone.0193006
Differences between fellow eyes of acute and chronic primary angle closure (glaucoma): An ultrasound biomicroscopy quantitative study
Abstract
Purpose: To compare various biometric parameters between fellow eyes of acute primary angle closure (glaucoma) [APAC(G)] and fellow eyes of chronic primary angle closure (glaucoma) [CPAC(G)].
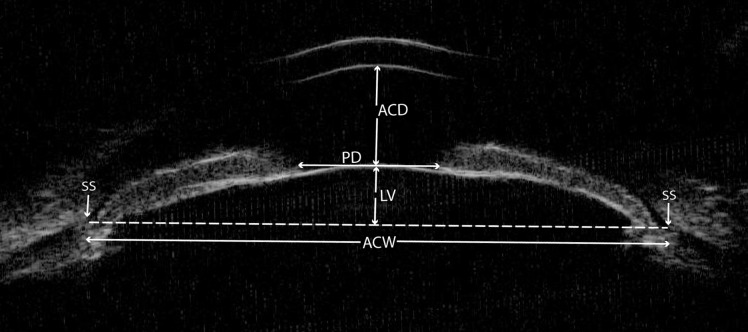
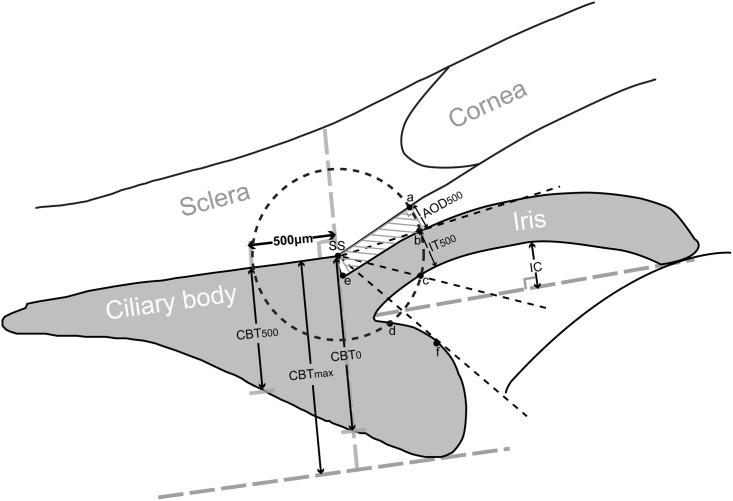
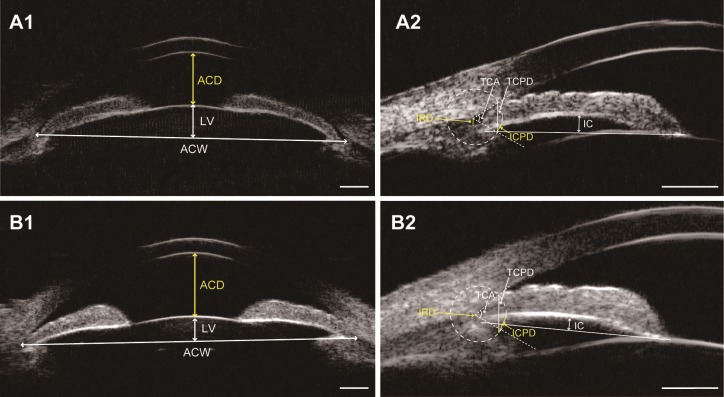
Methods: Ultrasound biomicroscopy examinations were performed on 47 patients with unilateral APAC(G) and 41 patients with asymmetric CPAC(G) before laser peripheral iridotomy and pilocarpine treatment. Anterior chamber depth and width (ACD and ACW), lens vault (LV), iris curvature (IC), iris root distance (IRD), trabecular-ciliary process distance (TCPD), iris-ciliary process distance (ICPD), trabecular-ciliary angle (TCA), and other biometric parameters were compared between fellow eyes of APAC(G) and fellow eyes of CAPC(G).
Results: Compared with fellow eyes of CPAC(G), fellow eyes of APAC(G) had smaller ACD (P < 0.001), ACW (P = 0.007), TCPD (P = 0.016), ICPD (P = 0.008), and TCA (P = 0.006), as well as larger LV (P = 0.002), IC (P = 0.012), and IRD (P = 0.003). On multivariate logistic regression analyses, a 0.1 mm decrease in ACD (odds ratio [OR]: 0.705, 95%CI: 0.564-0.880, P = 0.002), ICPD (OR: 0.557, 95%CI: 0.335-0.925, P = 0.024), and a 0.1 mm increase in IRD (OR: 2.707, 95%CI: 1.025-7.149, P = 0.045), was significantly associated with occurrence of acute angle closures.
Conclusions: Fellow eyes of APAC(G) had smaller anterior segment dimensions, higher LV, more posterior iris insertion, greater IC, and more anteriorly rotated ciliary body compared with fellow eyes of CPAC(G). ACD, ICPD, and IRD were the three most important parameters that distinguish eyes predisposed to APAC(G) or CPAC(G).
Conflict of interest statement
Figures
References
-
- Foster PJ, Johnson GJ. Glaucoma in China: How big is the problem? Br J Ophthalmol. 2001;85:1277–1282. doi: 10.1136/bjo.85.11.1277 - DOI - PMC - PubMed
-
- Sun X, Dai Y, Chen Y, Yu DY, Cringle SJ, Chen J, et al. Primary angle closure glaucoma: What we know and what we don't know. Prog Retin Eye Res. 2017;57:26–45. doi: 10.1016/j.preteyeres.2016.12.003 - DOI - PubMed
-
- Wright C, Tawfik MA, Waisbourd M, Katz LJ. Primary angle-closure glaucoma: An update. Acta Ophthalmol. 2016;94:217–225. doi: 10.1111/aos.12784 - DOI - PubMed
-
- Nongpiur ME, Ku JY, Aung T. Angle closure glaucoma: A mechanistic review. Curr Opin Ophthalmol. 2011;22:96–101. doi: 10.1097/ICU.0b013e32834372b9 - DOI - PubMed
-
- Nongpiur ME, He M, Amerasinghe N, Friedman DS, Tay WT, Baskaran M, et al. Lens vault, thickness, and position in Chinese subjects with angle closure. Ophthalmology. 2011;118:474–479. doi: 10.1016/j.ophtha.2010.07.025 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
