

Influenza interaction with cocirculating pathogens and its impact on surveillance, pathogenesis, and epidemic profile: A key role for mathematical modelling
- PMID: 29447284
- PMCID: PMC5814058
- DOI: 10.1371/journal.ppat.1006770
Influenza interaction with cocirculating pathogens and its impact on surveillance, pathogenesis, and epidemic profile: A key role for mathematical modelling
Abstract
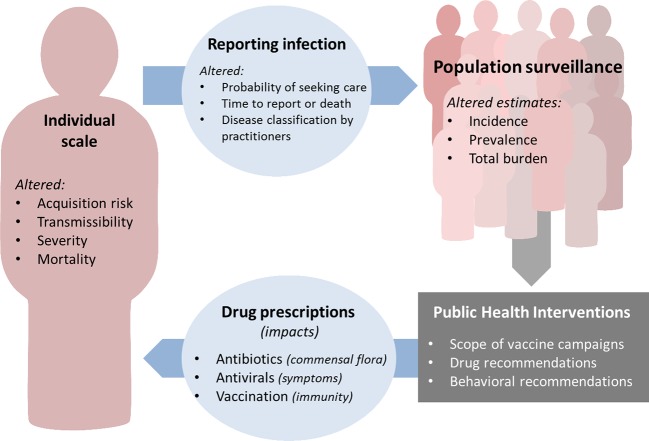
Evidence is mounting that influenza virus interacts with other pathogens colonising or infecting the human respiratory tract. Taking into account interactions with other pathogens may be critical to determining the real influenza burden and the full impact of public health policies targeting influenza. This is particularly true for mathematical modelling studies, which have become critical in public health decision-making. Yet models usually focus on influenza virus acquisition and infection alone, thereby making broad oversimplifications of pathogen ecology. Herein, we report evidence of influenza virus interactions with bacteria and viruses and systematically review the modelling studies that have incorporated interactions. Despite the many studies examining possible associations between influenza and Streptococcus pneumoniae, Staphylococcus aureus, Haemophilus influenzae, Neisseria meningitidis, respiratory syncytial virus (RSV), human rhinoviruses, human parainfluenza viruses, etc., very few mathematical models have integrated other pathogens alongside influenza. The notable exception is the pneumococcus-influenza interaction, for which several recent modelling studies demonstrate the power of dynamic modelling as an approach to test biological hypotheses on interaction mechanisms and estimate the strength of those interactions. We explore how different interference mechanisms may lead to unexpected incidence trends and possible misinterpretation, and we illustrate the impact of interactions on public health surveillance using simple transmission models. We demonstrate that the development of multipathogen models is essential to assessing the true public health burden of influenza and that it is needed to help improve planning and evaluation of control measures. Finally, we identify the public health, surveillance, modelling, and biological challenges and propose avenues of research for the coming years.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures



References
-
- Webster RG, Monto A. S., Braciale T. J. & Lamb R. A. (2013) Textbook of Influenza.
-
- Bosch AATM, Biesbroek G, Trzcinski K, Sanders EAM, Bogaert D (2013) Viral and bacterial interactions in the upper respiratory tract. PLoS Pathog 9: e1003057 doi: 10.1371/journal.ppat.1003057 - DOI - PMC - PubMed
-
- Yamin D, Balicer RD, Galvani AP (2014) Cost-effectiveness of influenza vaccination in prior pneumonia patients in Israel. Vaccine 32: 4198–4205. doi: 10.1016/j.vaccine.2014.05.015 - DOI - PMC - PubMed
-
- Bedford T, Riley S, Barr IG, Broor S, Chadha M, et al. (2015) Global circulation patterns of seasonal influenza viruses vary with antigenic drift. Nature 523: 217–220. doi: 10.1038/nature14460 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
