

Antimicrobial Prophylaxis with Combat-Related Open Soft-Tissue Injuries
- PMID: 29447384
- PMCID: PMC6089685
- DOI: 10.1093/milmed/usx125
Antimicrobial Prophylaxis with Combat-Related Open Soft-Tissue Injuries
Abstract
Introduction: All Department of Defense (DoD) guidance documents recommend cefazolin or clindamycin as post-trauma antibiotic prophylaxis for open soft-tissue injuries. Although not advocated, some patients with open soft-tissue injuries also received expanded Gram-negative coverage (EGN) prophylaxis based on the judgment of front-line trauma providers. During the study period, revised guidelines in 2011/2012 re-emphasized recommendations for using cefazolin or clindamycin, and stewardship efforts in the DoD trauma community aimed to reduce the practice of adding EGN to guideline-recommended antibiotic prophylaxis. Our objective was to examine antibiotic utilization among wounded military personnel with open extremity soft-tissue injuries over a 5-yr period and assess the impact on infectious outcomes in patients who received EGN prophylaxis versus guideline-directed prophylaxis.
Methods: The study population included military personnel with open extremity soft-tissue injuries sustained in Iraq and Afghanistan (2009-2014) who transferred to participating hospitals in the USA following medical evacuation. The analysis was restricted to patients who were hospitalized for at least seven days at a U.S. facility and excluded those who sustained open fractures. Post-trauma antibiotic prophylactic regimens were defined as narrow if they followed recommended guidance (e.g., IV cefazolin or clindamycin) or EGN coverage when the narrow regimen also included fluoroquinolones and/or aminoglycosides. Intravenous amoxicillin-clavulanate, which is commonly used at non-U.S. coalition theater hospitals, was also classified as narrow because it conformed to coalition antibiotic prophylaxis guidelines. This study was approved by the Infectious Disease Institutional Review Board of the Uniformed Services University of the Health Sciences.
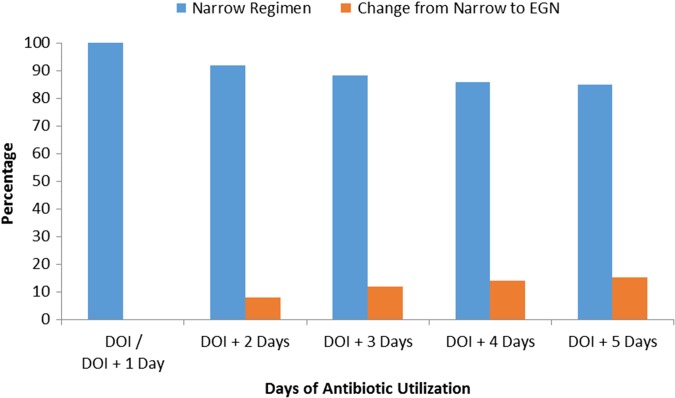
Results: A total of 287 wounded personnel with open soft-tissue injuries were assessed, of which 212 (74%) received narrow prophylaxis and 75 (26%) received EGN coverage (p < 0.001). Among patients in the narrow prophylaxis group, 81% were given cefazolin and/or clindamycin, while 19% received amoxicillin-clavulanate. In the EGN group, 88% and 12% received a fluoroquinolone and aminoglycoside, respectively. Use of EGN coverage significantly declined during the study period from 39% in 2009-2010 to 11% in 2013-2014 (p < 0.001). Approximately 3% of patients who received a narrow regimen developed an extremity skin and soft-tissue infection, while there were no skin and soft-tissue infections among patients in the EGN coverage group. Nonetheless, this was not a significant difference (p = 0.345). In addition, the proportion of non-extremity infections was not significantly different between narrow and EGN regimen groups (11% and 15%, respectively). There were also no significant differences between the narrow and EGN regimen groups related to duration of hospitalization (median of 19 versus 20 d).
Conclusion: Use of non-guideline directed EGN-based post-trauma antibiotic prophylaxis does not improve infectious outcomes nor does it shorten hospital stay.
Keywords: antimicrobial prophylaxis; clinical practice guidelines; combat-related infections; extremity infections; open soft-tissue injuries.
Published by Oxford University Press on behalf of the Association of Military Surgeons of the United States 2018.
Figures
Similar articles
-
After the Battlefield: Infectious Complications among Wounded Warriors in the Trauma Infectious Disease Outcomes Study.Mil Med. 2019 Nov 1;184(Suppl 2):18-25. doi: 10.1093/milmed/usz027. Mil Med. 2019. PMID: 31778199 Free PMC article.
-
Department of Defense Trauma Registry Infectious Disease Module Impact on Clinical Practice.Mil Med. 2022 May 4;187(Suppl 2):7-16. doi: 10.1093/milmed/usac050. Mil Med. 2022. PMID: 35512379 Free PMC article. Review.
-
Early infectious outcomes after addition of fluoroquinolone or aminoglycoside to posttrauma antibiotic prophylaxis in combat-related open fracture injuries.J Trauma Acute Care Surg. 2017 Nov;83(5):854-861. doi: 10.1097/TA.0000000000001609. J Trauma Acute Care Surg. 2017. PMID: 28570348 Free PMC article.
-
Variation in Postinjury Antibiotic Prophylaxis Patterns Over Five Years in a Combat Zone.Mil Med. 2017 Mar;182(S1):346-352. doi: 10.7205/MILMED-D-16-00040. Mil Med. 2017. PMID: 28291497 Free PMC article.
-
IDCRP Combat-Related Extremity Wound Infection Research.Mil Med. 2022 May 4;187(Suppl 2):25-33. doi: 10.1093/milmed/usab065. Mil Med. 2022. PMID: 35512376 Free PMC article. Review.
Cited by
-
Enterobacter cloacae infection characteristics and outcomes in battlefield trauma patients.PLoS One. 2023 Aug 29;18(8):e0290735. doi: 10.1371/journal.pone.0290735. eCollection 2023. PLoS One. 2023. PMID: 37643169 Free PMC article.
-
Antibiotic Prophylaxis in Torso, Maxillofacial, and Skin Traumatic Lesions: A Systematic Review of Recent Evidence.Antibiotics (Basel). 2022 Jan 21;11(2):139. doi: 10.3390/antibiotics11020139. Antibiotics (Basel). 2022. PMID: 35203743 Free PMC article. Review.
-
Antibiotic Practice Patterns for Extremity Wound Infections among Blast-Injured Subjects.Mil Med. 2020 Jan 7;185(Suppl 1):628-636. doi: 10.1093/milmed/usz211. Mil Med. 2020. PMID: 32074316 Free PMC article.
-
After the Battlefield: Infectious Complications among Wounded Warriors in the Trauma Infectious Disease Outcomes Study.Mil Med. 2019 Nov 1;184(Suppl 2):18-25. doi: 10.1093/milmed/usz027. Mil Med. 2019. PMID: 31778199 Free PMC article.
-
Department of Defense Trauma Registry Infectious Disease Module Impact on Clinical Practice.Mil Med. 2022 May 4;187(Suppl 2):7-16. doi: 10.1093/milmed/usac050. Mil Med. 2022. PMID: 35512379 Free PMC article. Review.
References
-
- Hoff WS, Bonadies JA, Cachecho R, Dorlac WC: East Practice Management Guidelines Work Group: update to practice management guidelines for prophylactic antibiotic use in open fractures. J Trauma 2011; 70(3): 751–4. - PubMed
-
- Jaeger M, Maier D, Kern WV, Sudkamp NP: Antibiotics in trauma and orthopedic surgery – a primer of evidence-based recommendations. Injury 2006; 37(Suppl 2): S74–80. - PubMed
-
- Hauser CJ, Adams CA Jr., Eachempati SR: Council of the Surgical Infection Society: Surgical Infection Society guideline: prophylactic antibiotic use in open fractures: an evidence-based guideline. Surg Infect (Larchmt) 2006; 7(4): 379–405. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
