

Effectiveness of systemic family therapy versus treatment as usual for young people after self-harm: a pragmatic, phase 3, multicentre, randomised controlled trial
- PMID: 29449180
- PMCID: PMC5835764
- DOI: 10.1016/S2215-0366(18)30058-0
Effectiveness of systemic family therapy versus treatment as usual for young people after self-harm: a pragmatic, phase 3, multicentre, randomised controlled trial
Abstract
Background: Self-harm in adolescents is common and repetition occurs in a high proportion of these cases. Scarce evidence exists for effectiveness of interventions to reduce self-harm.
Methods: This pragmatic, multicentre, randomised, controlled trial of family therapy versus treatment as usual was done at 40 UK Child and Adolescent Mental Health Services (CAMHS) centres. We recruited young people aged 11-17 years who had self-harmed at least twice and presented to CAMHS after self-harm. Participants were randomly assigned (1:1) to receive manualised family therapy delivered by trained and supervised family therapists or treatment as usual by local CAMHS. Participants and therapists were aware of treatment allocation; researchers were masked. The primary outcome was hospital attendance for repetition of self-harm in the 18 months after group assignment. Primary and safety analyses were done in the intention-to-treat population. The trial is registered at the ISRCTN registry, number ISRCTN59793150.
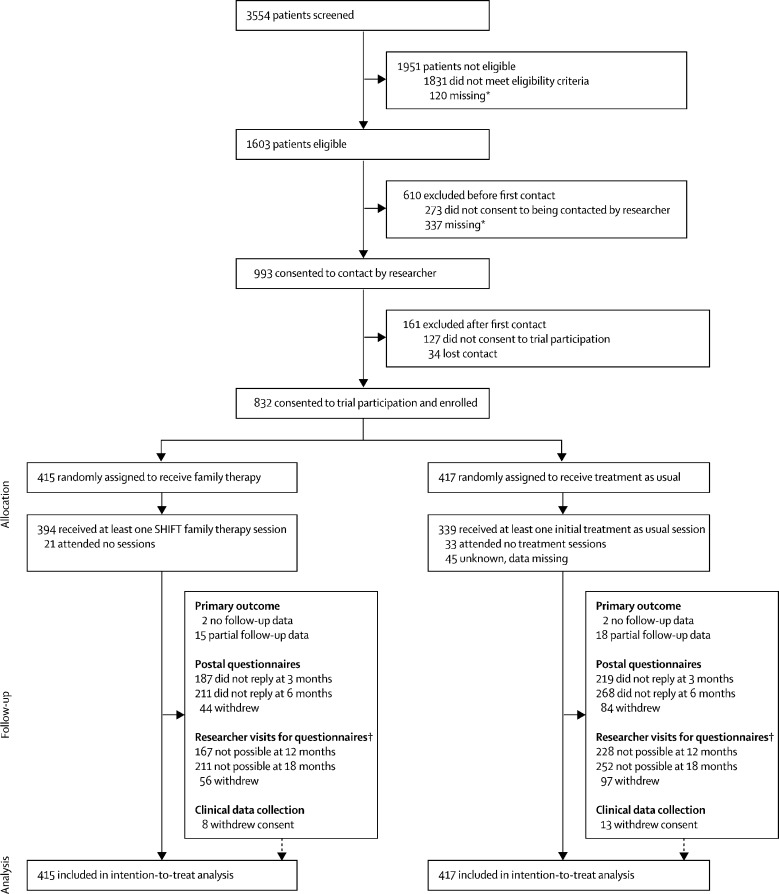
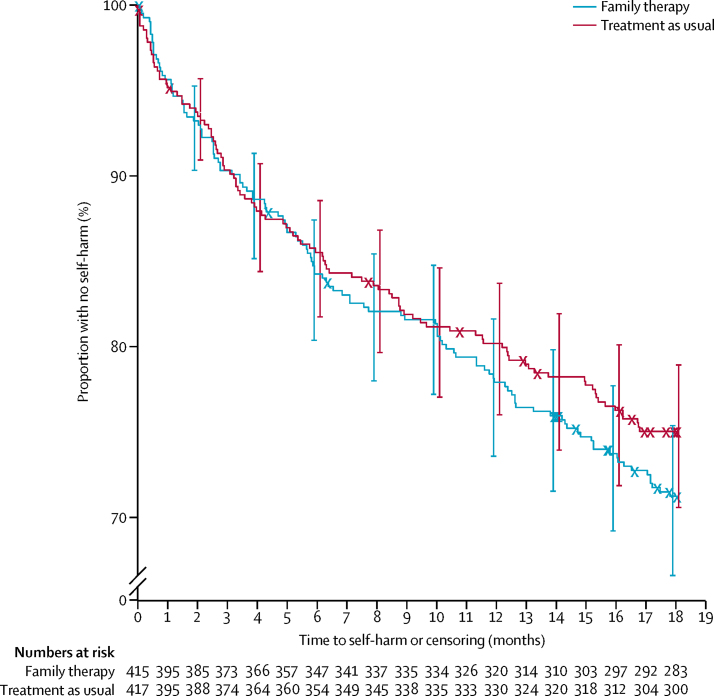
Findings: Between Nov 23, 2009, and Dec 31, 2013, 3554 young people were screened and 832 eligible young people consented to participation and were randomly assigned to receive family therapy (n=415) or treatment as usual (n=417). Primary outcome data were available for 795 (96%) participants. Numbers of hospital attendances for repeat self-harm events were not significantly different between the groups (118 [28%] in the family therapy group vs 103 [25%] in the treatment as usual group; hazard ratio 1·14 [95% CI 0·87-1·49] p=0·33). Similar numbers of adverse events occurred in both groups (787 in the family therapy group vs 847 in the treatment as usual group).
Interpretation: For adolescents referred to CAMHS after self-harm, having self-harmed at least once before, our family therapy intervention conferred no benefits over treatment as usual in reducing subsequent hospital attendance for self-harm. Clinicians are therefore still unable to recommend a clear, evidence-based intervention to reduce repeated self-harm in adolescents.
Funding: National Institute for Health Research Health Technology Assessment programme.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
The end of family therapy for self-harm, or a new beginning?Lancet Psychiatry. 2018 Mar;5(3):188-189. doi: 10.1016/S2215-0366(18)30043-9. Epub 2018 Feb 12. Lancet Psychiatry. 2018. PMID: 29449179 No abstract available.
-
Systemic family therapy is not superior to treatment as usual in preventing repeat self-harm in adolescents.Evid Based Ment Health. 2019 May;22(2):e9. doi: 10.1136/ebmental-2018-300056. Epub 2019 Mar 2. Evid Based Ment Health. 2019. PMID: 30826749 Free PMC article. No abstract available.
References
-
- Evans E, Hawton K, Rodham K, Deeks J. The prevalence of suicidal phenomena in adolescents: a systematic review of population-based studies. Suicide Life Threat Behav. 2005;35:239–250. - PubMed
-
- Hawton K, Saunders KE, O'Connor RC. Self-harm and suicide in adolescents. Lancet. 2012;379:2373–2382. - PubMed
-
- Hawton K, Harriss L. Deliberate self-harm in young people: characteristics and subsequent mortality in a 20-year cohort of patients presenting to hospital. J Clin Psychiatry. 2007;68:1574–1583. - PubMed
-
- Hawton K, Bergen H, Kapur N. Repetition of self-harm and suicide following self-harm in children and adolescents: findings from the Multicentre Study of Self-harm in England. J Child Psychol Psychiatry. 2012;53:1212–1219. - PubMed
-
- Hawton K, Bergen H, Waters K. Epidemiology and nature of self-harm in children and adolescents: findings from the multicentre study of self-harm in England. Eur Child Adolesc Psychiatry. 2012;21:369–377. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
