

Adjuvant chemoradiotherapy versus radiotherapy alone for women with high-risk endometrial cancer (PORTEC-3): final results of an international, open-label, multicentre, randomised, phase 3 trial
- PMID: 29449189
- PMCID: PMC5840256
- DOI: 10.1016/S1470-2045(18)30079-2
Adjuvant chemoradiotherapy versus radiotherapy alone for women with high-risk endometrial cancer (PORTEC-3): final results of an international, open-label, multicentre, randomised, phase 3 trial
Erratum in
-
Correction to Lancet Oncol 2018; 19: 295-309.Lancet Oncol. 2018 Apr;19(4):e184. doi: 10.1016/S1470-2045(18)30212-2. Lancet Oncol. 2018. PMID: 29611526 Free PMC article. No abstract available.
Abstract
Background: Although women with endometrial cancer generally have a favourable prognosis, those with high-risk disease features are at increased risk of recurrence. The PORTEC-3 trial was initiated to investigate the benefit of adjuvant chemotherapy during and after radiotherapy (chemoradiotherapy) versus pelvic radiotherapy alone for women with high-risk endometrial cancer.
Methods: PORTEC-3 was an open-label, international, randomised, phase 3 trial involving 103 centres in six clinical trials collaborating in the Gynaecological Cancer Intergroup. Eligible women had high-risk endometrial cancer with FIGO 2009 stage I, endometrioid-type grade 3 with deep myometrial invasion or lymph-vascular space invasion (or both), endometrioid-type stage II or III, or stage I to III with serous or clear cell histology. Women were randomly assigned (1:1) to receive radiotherapy alone (48·6 Gy in 1·8 Gy fractions given on 5 days per week) or radiotherapy and chemotherapy (consisting of two cycles of cisplatin 50 mg/m2 given during radiotherapy, followed by four cycles of carboplatin AUC5 and paclitaxel 175 mg/m2) using a biased-coin minimisation procedure with stratification for participating centre, lymphadenectomy, stage of cancer, and histological type. The co-primary endpoints were overall survival and failure-free survival. We used the Kaplan-Meier method, log-rank test, and Cox regression analysis for final analysis by intention to treat and adjusted for stratification factors. The study was closed on Dec 20, 2013, after achieving complete accrual; follow-up is ongoing. PORTEC-3 is registered with ISRCTN, number ISRCTN14387080, and ClinicalTrials.gov, number NCT00411138.
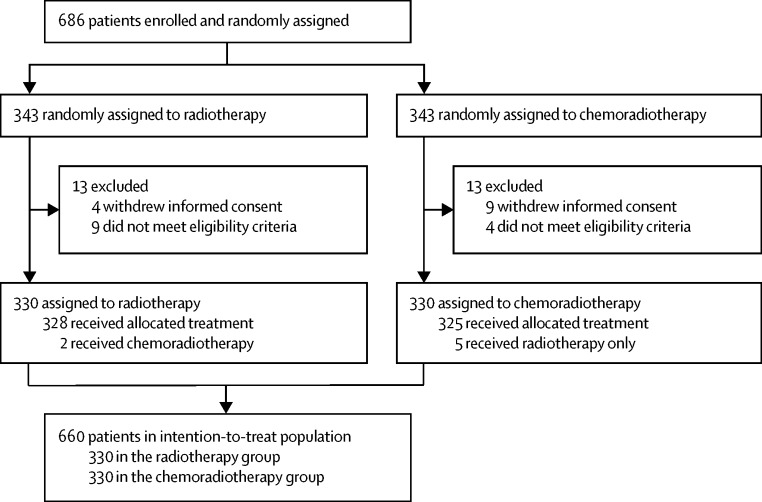
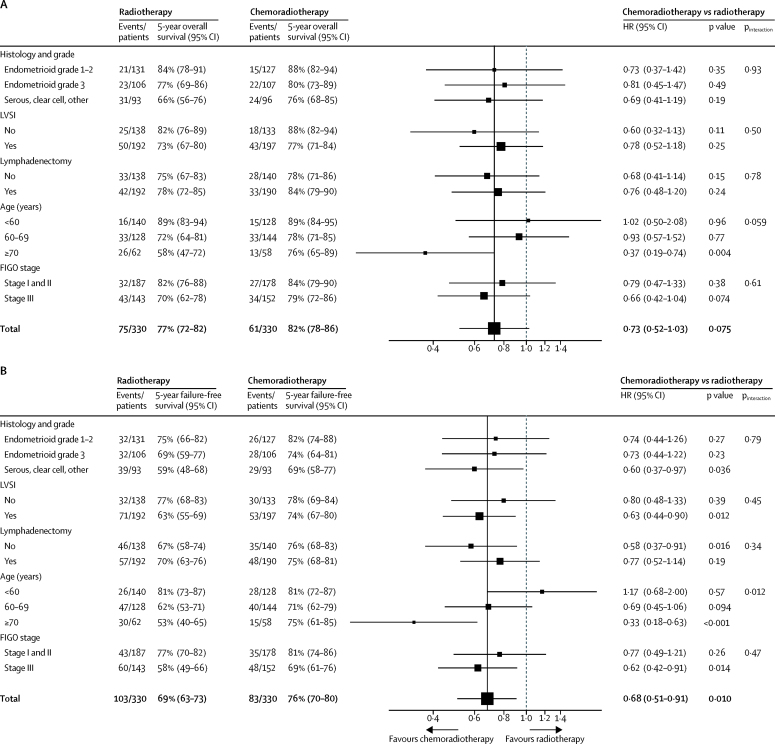
Results: 686 women were enrolled between Nov 23, 2006, and Dec 20, 2013. 660 eligible patients were included in the final analysis, of whom 330 were assigned to chemoradiotherapy and 330 were assigned to radiotherapy. Median follow-up was 60·2 months (IQR 48·1-73·1). 5-year overall survival was 81·8% (95% CI 77·5-86·2) with chemoradiotherapy versus 76·7% (72·1-81·6) with radiotherapy (adjusted hazard ratio [HR] 0·76, 95% CI 0·54-1·06; p=0·11); 5-year failure-free survival was 75·5% (95% CI 70·3-79·9) versus 68·6% (63·1-73·4; HR 0·71, 95% CI 0·53-0·95; p=0·022). Grade 3 or worse adverse events during treatment occurred in 198 (60%) of 330 who received chemoradiotherapy versus 41 (12%) of 330 patients who received radiotherapy (p<0·0001). Neuropathy (grade 2 or worse) persisted significantly more often after chemoradiotherapy than after radiotherapy (20 [8%] women vs one [1%] at 3 years; p<0·0001). Most deaths were due to endometrial cancer; in four patients (two in each group), the cause of death was uncertain. One death in the radiotherapy group was due to either disease progression or late treatment complications; three deaths (two in the chemoradiotherapy group and one in the radiotherapy group) were due to either intercurrent disease or late treatment-related toxicity.
Interpretation: Adjuvant chemotherapy given during and after radiotherapy for high-risk endometrial cancer did not improve 5-year overall survival, although it did increase failure-free survival. Women with high-risk endometrial cancer should be individually counselled about this combined treatment. Continued follow-up is needed to evaluate long-term survival.
Funding: Dutch Cancer Society, Cancer Research UK, National Health and Medical Research Council Project Grant and Cancer Australia, L'Agenzia Italiana del Farmaco, and Canadian Cancer Society Research Institute.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC-BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures

Comment in
-
Adjuvant therapy for women with high-risk endometrial carcinoma.Lancet Oncol. 2018 Mar;19(3):268-269. doi: 10.1016/S1470-2045(18)30091-3. Epub 2018 Feb 12. Lancet Oncol. 2018. PMID: 29449190 No abstract available.
-
[High-risk endometrial cancer: In each case an adjuvant radiochemotherapy?].Strahlenther Onkol. 2018 Oct;194(10):960-961. doi: 10.1007/s00066-018-1351-x. Strahlenther Onkol. 2018. PMID: 30143813 German. No abstract available.
-
Defining the Place of Adjuvant Chemotherapy and Radiation for High-Risk Endometrial Cancer From Recent Randomized Clinical Trials: Some Answers, More Questions.Int J Radiat Oncol Biol Phys. 2018 Nov 1;102(3):473-477. doi: 10.1016/j.ijrobp.2018.05.034. Int J Radiat Oncol Biol Phys. 2018. PMID: 30238893 No abstract available.
-
[The PORTEC-3 trial for high-risk endometrial cancer: impact of molecular classification on prognosis and benefit from adjuvant therapy].Strahlenther Onkol. 2021 Mar;197(3):266-268. doi: 10.1007/s00066-020-01735-4. Epub 2021 Jan 5. Strahlenther Onkol. 2021. PMID: 33403442 German. No abstract available.
References
-
- Straughn JM, Huh WK, Orr JW., Jr Stage IC adenocarcinoma of the endometrium: survival comparisons of surgically staged patients with and without adjuvant radiation therapy. Gynecol Oncol. 2003;89:295–300. - PubMed
-
- Greven KM, Randall M, Fanning J. Patterns of failure in patients with stage I, grade 3 carcinoma of the endometrium. Int J Radiat Oncol Biol Phys. 1990;19:529–534. - PubMed
-
- Creutzberg CL, van Putten WL, Warlam-Rodenhuis CC. Outcome of high-risk stage IC, grade 3, compared with stage I endometrial carcinoma patients: the postoperative radiation therapy in endometrial carcinoma trial. J Clin Oncol. 2004;22:1234–1241. - PubMed
-
- Bosse T, Peters EE, Creutzberg CL. Substantial lymph-vascular space invasion (LVSI) is a significant risk factor for recurrence in endometrial cancer—a pooled analysis of PORTEC 1 and 2 trials. Eur J Cancer. 2015;51:1742–1750. - PubMed
-
- Creasman WT, Kohler MF, Odicino F, Maisonneuve P, Boyle P. Prognosis of papillary serous, clear cell, and grade 3 stage I carcinoma of the endometrium. Gynecol Oncol. 2004;95:593–596. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
