

Common surgical procedures in pilonidal sinus disease: A meta-analysis, merged data analysis, and comprehensive study on recurrence
- PMID: 29449548
- PMCID: PMC5814421
- DOI: 10.1038/s41598-018-20143-4
Common surgical procedures in pilonidal sinus disease: A meta-analysis, merged data analysis, and comprehensive study on recurrence
Abstract
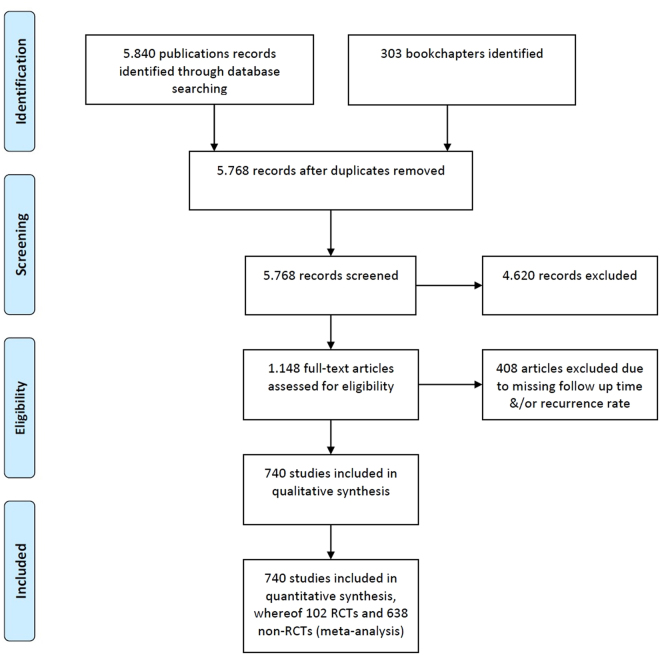
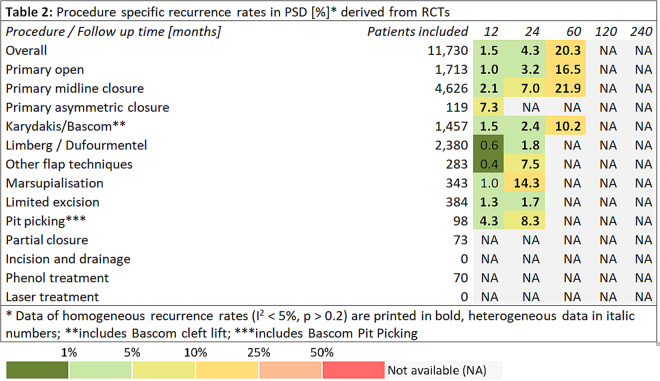
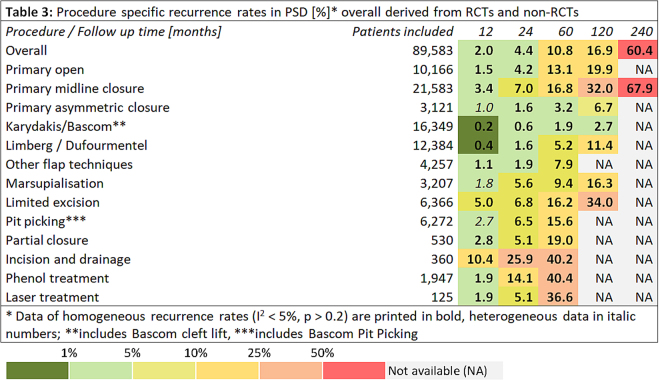
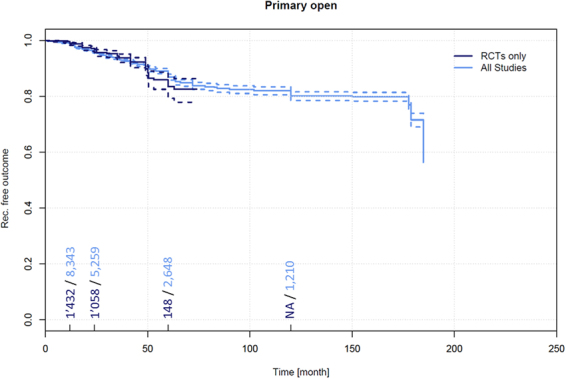
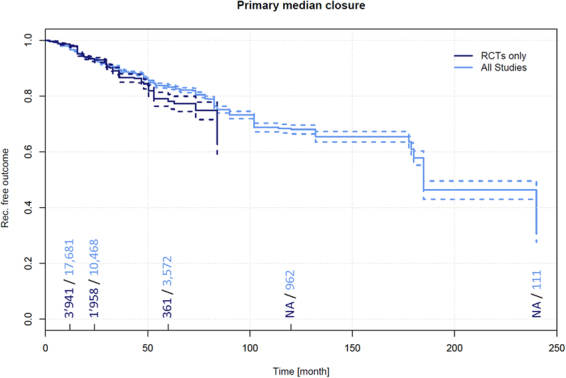
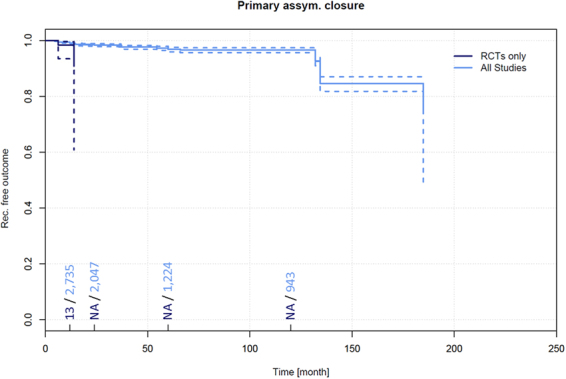
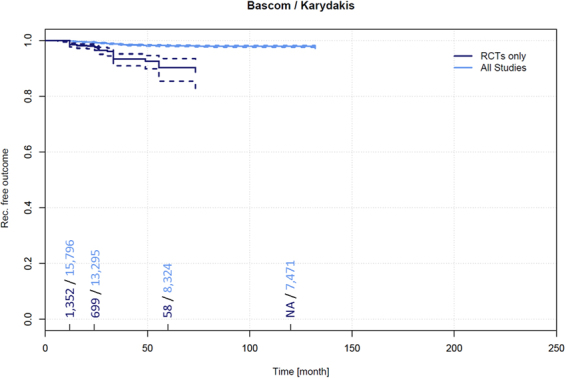
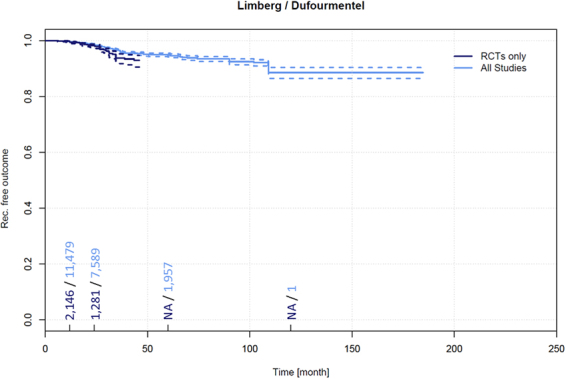
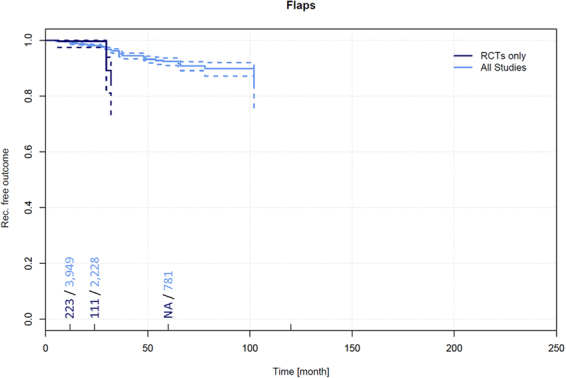
We systematically searched available databases. We reviewed 6,143 studies published from 1833 to 2017. Reports in English, French, German, Italian, and Spanish were considered, as were publications in other languages if definitive treatment and recurrence at specific follow-up times were described in an English abstract. We assessed data in the manner of a meta-analysis of RCTs; further we assessed non-RCTs in the manner of a merged data analysis. In the RCT analysis including 11,730 patients, Limberg & Dufourmentel operations were associated with low recurrence of 0.6% (95%CI 0.3-0.9%) 12 months and 1.8% (95%CI 1.1-2.4%) respectively 24 months postoperatively. Analysing 89,583 patients from RCTs and non-RCTs, the Karydakis & Bascom approaches were associated with recurrence of only 0.2% (95%CI 0.1-0.3%) 12 months and 0.6% (95%CI 0.5-0.8%) 24 months postoperatively. Primary midline closure exhibited long-term recurrence up to 67.9% (95%CI 53.3-82.4%) 240 months post-surgery. For most procedures, only a few RCTs without long term follow up data exist, but substitute data from numerous non-RCTs are available. Recurrence in PSD is highly dependent on surgical procedure and by follow-up time; both must be considered when drawing conclusions regarding the efficacy of a procedure.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Evers T, et al. Trends in incidence and long-term recurrence rate of pilonidal sinus disease and analysis of associated influencing factors. Zhonghua Wai Ke Za Zhi. 2011;49:799–803. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
