

Nutritional rickets in immigrant and refugee children
- PMID: 29450045
- PMCID: PMC5810111
- DOI: 10.1186/s40985-016-0018-3
Nutritional rickets in immigrant and refugee children
Abstract
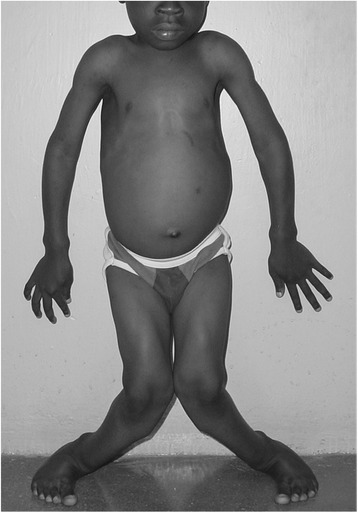
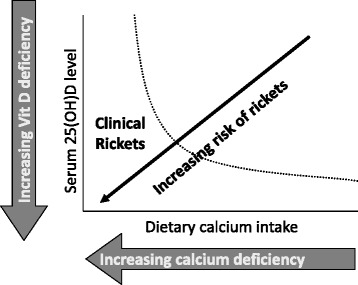
Immigrant and refugee populations bring public health challenges to host nations. In the current global refugee crisis, children are the most vulnerable subpopulation. Diseases that were considered rare in the host nation may be highly prevalent among immigrant children. The prevalence of nutritional rickets is increasing in high-income countries, largely driven by an influx of immigrant populations. Nutritional rickets is a bone disease in early childhood resulting in bone pain, delayed motor development, and bending of the bones, caused by vitamin D deficiency and/or inadequate dietary calcium intake. The consequences of nutritional rickets include stunted growth, developmental delay, lifelong bone deformities, seizures, cardiomyopathy, and even death. Nutritional rickets is most commonly seen in children from the Middle East, Africa, and South Asia in high-income countries. Dark skin pigmentation, sun avoidance, covering the skin, and prolonged breast feeding without vitamin D supplementation, are important risk factors for vitamin D deficiency, and combined with a lack of dairy products in the diet, these deficiencies can result in insufficient calcium supply for bone mineralization. We recommend screening all immigrant and refugee children under 5 years of age from these ethnic groups for nutritional rickets, based on clinical features, and confirming the diagnosis with radiographs of the wrists and knees. Because nutritional rickets is entirely preventable, public health policies must address the need for universal vitamin D supplementation and adequate dietary calcium to protect children from this scourge. Vitamin D supplementation of all infants and children with 400 IU/d during the first year of life and dietary or supplemental intakes of at least 600 IU/d of vitamin D and 500 mg/d of calcium thereafter, will effectively prevent nutritional rickets. We call on national health authorities of host countries to implement health check lists and prevention programs that include screening for micronutrient deficiencies, in addition to assessing infections and vaccination programs. Due to their high prevalence of vitamin D deficiency, refugee children of all ages from these ethnic groups should be supplemented with vitamin D, beginning upon arrival.
Keywords: Calcium; Metabolic bone; Nutrition; Pediatric; Vitamin D.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
