

Cardiac disease in children and young adults with various lysosomal storage diseases: Comparison of echocardiographic and ECG changes among clinical groups
- PMID: 29450157
- PMCID: PMC5801096
- DOI: 10.1016/j.ijchv.2013.10.002
Cardiac disease in children and young adults with various lysosomal storage diseases: Comparison of echocardiographic and ECG changes among clinical groups
Abstract
Background: Lysosomal storage disease (LSD) is a rare inherited disease group. Consecutively there are few data on cardiac changes in mucopolysaccharidosis (MPS), Anderson Fabry disease (AFD), and other LSD (oLSD) including Pompe disease (PD) and Danon disease (DD), I-cell disease ICD and mucolipidosis III (ML III).
Methods: Between 1994 and 2011, we identified 39 patients with LSD: 25 with MPS, 8 with AFD, and 6 with oLSD including PD (1), ML III (2), DD (1), and ICD (2) at our institution fulfilling the inclusion criteria of at least one echocardiogram and ECG.
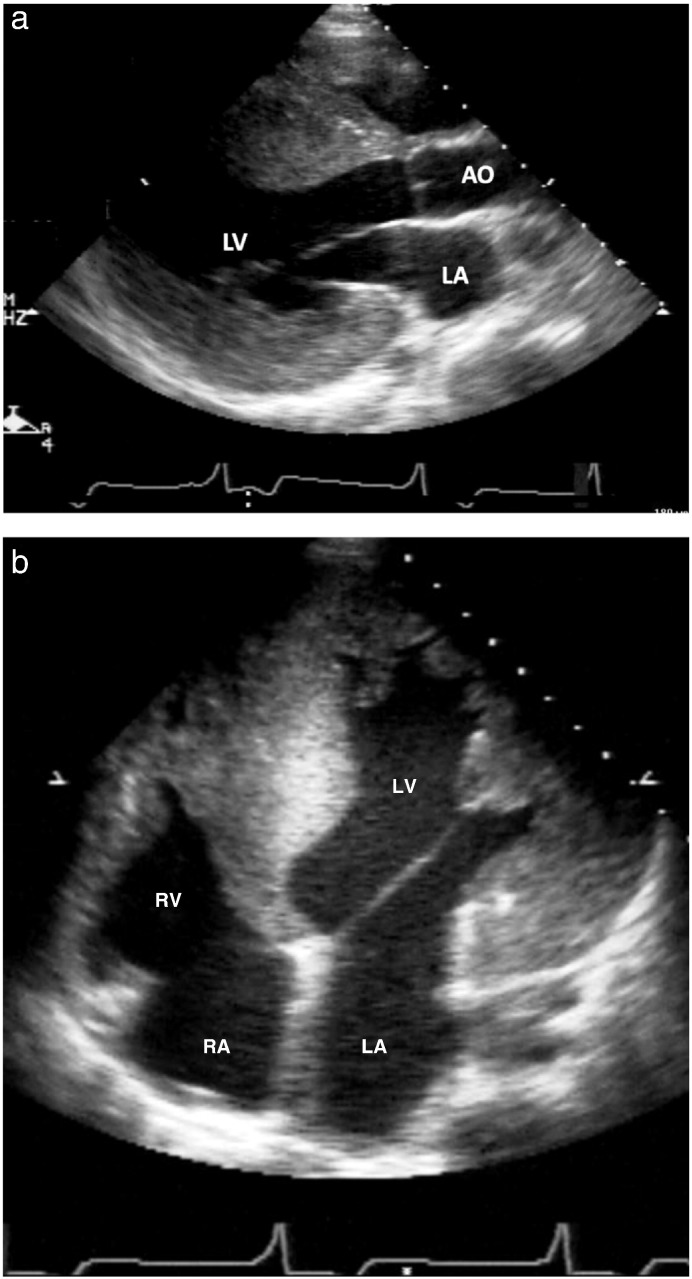
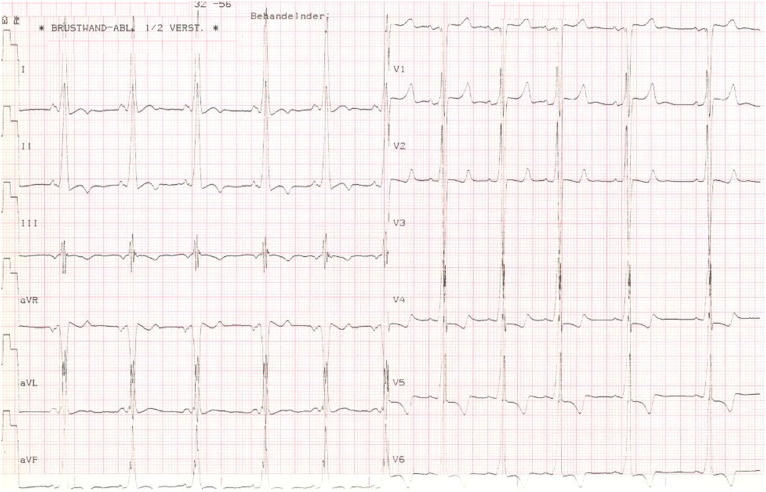
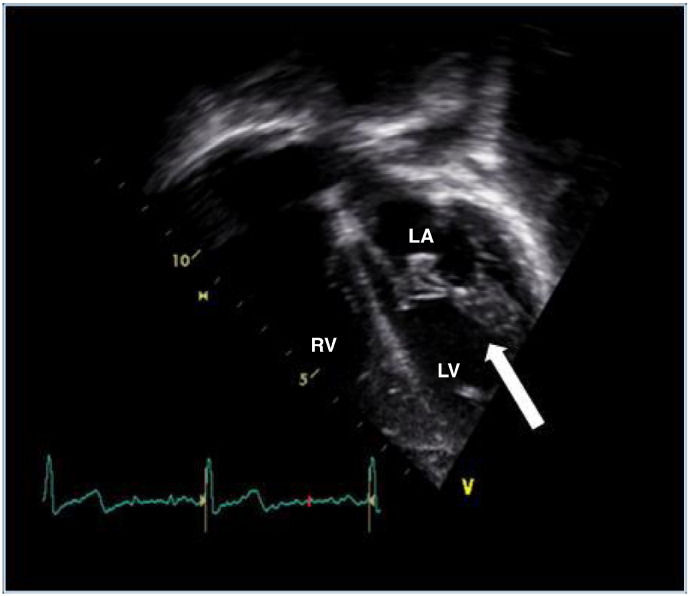
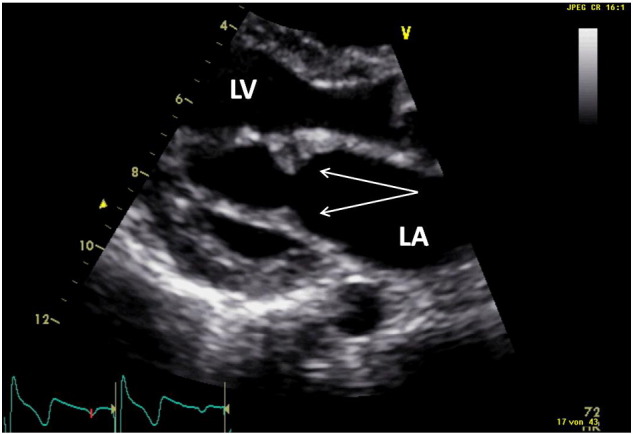
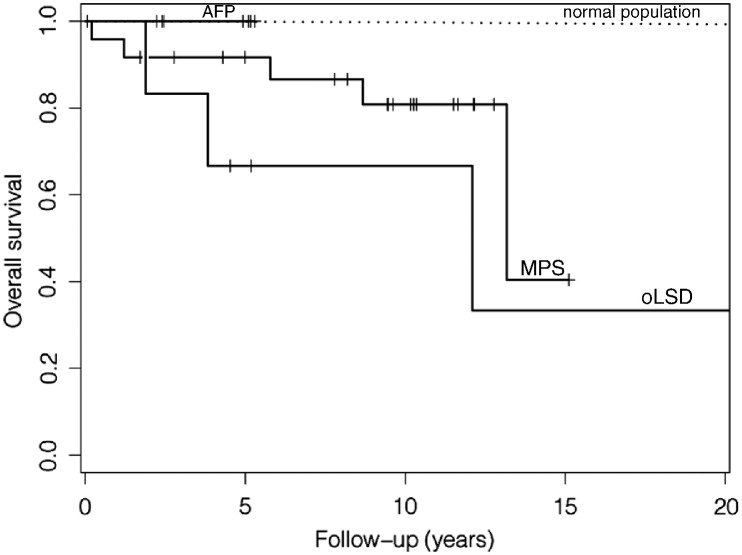
Results: Median age was 11.4 years (range: 2-27), 22 were females (56%). Normal echocardiograms were present in 12 patients (31%): 4 with MPS (16%), 7 AFD (88%), and 1 oLSD (17%). Valvular heart disease was present in 23 patients (59%) occurring more often in MPS (76%) and oLSD (67%) than in AFD (0%) (p < 0.001). The most common ECG abnormality was a short PR interval in 10 of 35 patients (29%) occurring in all LSD groups. Median follow-up was 5.8 (0.2-22.2) years showing diminished 5-year survival compared to an age-matched group. However, no patient died due to a cardiac cause and no cardiovascular intervention was necessary.
Conclusion: Echocardiographically detectable cardiovascular involvement in children with LSD is mostly confined to MPS and oLSD. Valve thickening in echo and a short PR interval in the ECG are the most frequent abnormalities. Routine repeat assessment is recommended in LSD. However, significant cardiac disease necessitating cardiac intervention is rare during a short follow-up.
Keywords: Anderson Fabry; Cardiovascular involvement; Lysosomal storage disease; Mucopolysaccharidosis.
Figures
Similar articles
-
Natural history of echocardiographic abnormalities in mucopolysaccharidosis III.Mol Genet Metab. 2018 Jun;124(2):131-134. doi: 10.1016/j.ymgme.2018.04.010. Epub 2018 Apr 27. Mol Genet Metab. 2018. PMID: 29735373 Free PMC article.
-
Aortopathies in mouse models of Pompe, Fabry and Mucopolysaccharidosis IIIB lysosomal storage diseases.PLoS One. 2020 May 19;15(5):e0233050. doi: 10.1371/journal.pone.0233050. eCollection 2020. PLoS One. 2020. PMID: 32428018 Free PMC article.
-
Cardiac manifestations of Anderson-Fabry disease in heterozygous females.J Am Coll Cardiol. 2002 Nov 6;40(9):1668-74. doi: 10.1016/s0735-1097(02)02380-x. J Am Coll Cardiol. 2002. PMID: 12427421
-
Cardiac involvement in Lysosomal Storage Diseases.J Biol Regul Homeost Agents. 2020 Jul-Aug;34(4 Suppl. 2):107-119. SPECIAL ISSUE: FOCUS ON PEDIATRIC CARDIOLOGY. J Biol Regul Homeost Agents. 2020. PMID: 33000609 Review.
-
Role of cardiac imaging in Anderson-Fabry cardiomyopathy.Cardiovasc Ultrasound. 2019 Jan 23;17(1):1. doi: 10.1186/s12947-019-0151-5. Cardiovasc Ultrasound. 2019. PMID: 30674321 Free PMC article. Review.
Cited by
-
Metabolic Cardiomyopathies and Cardiac Defects in Inherited Disorders of Carbohydrate Metabolism: A Systematic Review.Int J Mol Sci. 2023 May 11;24(10):8632. doi: 10.3390/ijms24108632. Int J Mol Sci. 2023. PMID: 37239976 Free PMC article.
-
Inappropriate cathepsin K secretion promotes its enzymatic activation driving heart and valve malformation.JCI Insight. 2020 Oct 15;5(20):e133019. doi: 10.1172/jci.insight.133019. JCI Insight. 2020. PMID: 33055423 Free PMC article.
-
Cardioprotective effects of CoQ10 in pediatric patients with lysosomal storage disorders.Ital J Pediatr. 2025 May 28;51(1):163. doi: 10.1186/s13052-025-02008-5. Ital J Pediatr. 2025. PMID: 40437590 Free PMC article.
-
A Prospective Treatment Option for Lysosomal Storage Diseases: CRISPR/Cas9 Gene Editing Technology for Mutation Correction in Induced Pluripotent Stem Cells.Diseases. 2017 Feb 24;5(1):6. doi: 10.3390/diseases5010006. Diseases. 2017. PMID: 28933359 Free PMC article. Review.
-
Metabolic Disorders and Anesthesia.Curr Anesthesiol Rep. 2019 Sep;9(3):340-359. doi: 10.1007/s40140-019-00345-w. Epub 2019 Jul 12. Curr Anesthesiol Rep. 2019. PMID: 31406490 Free PMC article.
References
-
- Wappner R.S. Lysosomal storage disorders. In: McMillan J.A., Feigin R.D., editors. Oski's pediatrics. Principles and practice. Lippincott Williams & Wilkins; Phildelphia: 2006. p. 2199.
-
- Meikle P.J., Hopwood J.J., Clague A.E., Carey W.F. Prevalence of lysosomal storage disorders. JAMA. 1999;281(3):249–254. - PubMed
-
- Hopwood J.J., Morris C.P. The mucopolysaccharidoses. Diagnosis, molecular genetics and treatment. Mol Biol Med. 1990;7(5):381–404. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials