

Effect of the Pulmonary Embolism Rule-Out Criteria on Subsequent Thromboembolic Events Among Low-Risk Emergency Department Patients: The PROPER Randomized Clinical Trial
- PMID: 29450523
- PMCID: PMC5838786
- DOI: 10.1001/jama.2017.21904
Effect of the Pulmonary Embolism Rule-Out Criteria on Subsequent Thromboembolic Events Among Low-Risk Emergency Department Patients: The PROPER Randomized Clinical Trial
Abstract
Importance: The safety of the pulmonary embolism rule-out criteria (PERC), an 8-item block of clinical criteria aimed at ruling out pulmonary embolism (PE), has not been assessed in a randomized clinical trial.
Objective: To prospectively validate the safety of a PERC-based strategy to rule out PE.
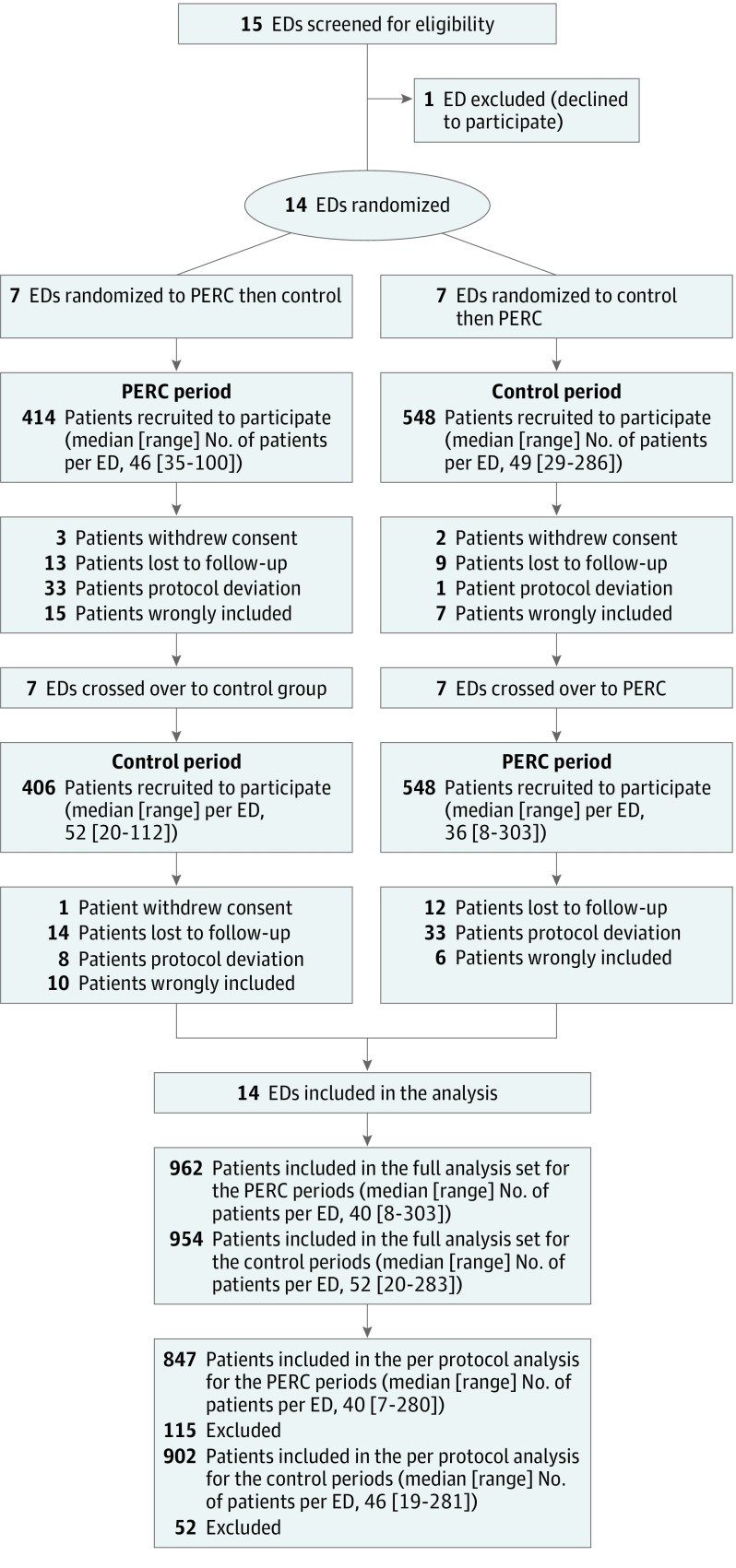
Design, setting, and patients: A crossover cluster-randomized clinical noninferiority trial in 14 emergency departments in France. Patients with a low gestalt clinical probability of PE were included from August 2015 to September 2016, and followed up until December 2016.
Interventions: Each center was randomized for the sequence of intervention periods. In the PERC period, the diagnosis of PE was excluded with no further testing if all 8 items of the PERC rule were negative.
Main outcomes and measures: The primary end point was the occurrence of a thromboembolic event during the 3-month follow-up period that was not initially diagnosed. The noninferiority margin was set at 1.5%. Secondary end points included the rate of computed tomographic pulmonary angiography (CTPA), median length of stay in the emergency department, and rate of hospital admission.
Results: Among 1916 patients who were cluster-randomized (mean age 44 years, 980 [51%] women), 962 were assigned to the PERC group and 954 were assigned to the control group. A total of 1749 patients completed the trial. A PE was diagnosed at initial presentation in 26 patients in the control group (2.7%) vs 14 (1.5%) in the PERC group (difference, 1.3% [95% CI, -0.1% to 2.7%]; P = .052). One PE (0.1%) was diagnosed during follow-up in the PERC group vs none in the control group (difference, 0.1% [95% CI, -∞ to 0.8%]). The proportion of patients undergoing CTPA in the PERC group vs control group was 13% vs 23% (difference, -10% [95% CI, -13% to -6%]; P < .001). In the PERC group, rates were significantly reduced for the median length of emergency department stay (mean reduction, 36 minutes [95% CI, 4 to 68]) and hospital admission (difference, 3.3% [95% CI, 0.1% to 6.6%]).
Conclusions and relevance: Among very low-risk patients with suspected PE, randomization to a PERC strategy vs conventional strategy did not result in an inferior rate of thromboembolic events over 3 months. These findings support the safety of PERC for very low-risk patients presenting to the emergency department.
Trial registration: clinicaltrials.gov Identifier: NCT02375919.
Conflict of interest statement
Figures
Comment in
-
Utility of a Clinical Prediction Rule to Exclude Pulmonary Embolism Among Low-Risk Emergency Department Patients: Reason to PERC Up.JAMA. 2018 Feb 13;319(6):551-553. doi: 10.1001/jama.2017.21901. JAMA. 2018. PMID: 29450510 No abstract available.
-
PERC strategy was noninferior to the usual strategy for ruling out PE in low-risk patients in the ED.Ann Intern Med. 2018 May 15;168(10):JC54. doi: 10.7326/ACPJC-2018-168-10-054. Ann Intern Med. 2018. PMID: 29800430 No abstract available.
References
-
- Konstantinides SV, Torbicki A, Agnelli G, et al. . 2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35(43):3033-3069, 3069a-3069k.. - PubMed
-
- van Belle A, Büller HR, Huisman MV, et al. ; Christopher Study Investigators . Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA. 2006;295(2):172-179. - PubMed
-
- Kline JA, Mitchell AM, Kabrhel C, Richman PB, Courtney DM. Clinical criteria to prevent unnecessary diagnostic testing in emergency department patients with suspected pulmonary embolism. J Thromb Haemost. 2004;2(8):1247-1255. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
