

Effect of a Quality Improvement Intervention on Clinical Outcomes in Patients in India With Acute Myocardial Infarction: The ACS QUIK Randomized Clinical Trial
- PMID: 29450524
- PMCID: PMC5838631
- DOI: 10.1001/jama.2017.21906
Effect of a Quality Improvement Intervention on Clinical Outcomes in Patients in India With Acute Myocardial Infarction: The ACS QUIK Randomized Clinical Trial
Abstract
Importance: Wide heterogeneity exists in acute myocardial infarction treatment and outcomes in India.
Objective: To evaluate the effect of a locally adapted quality improvement tool kit on clinical outcomes and process measures in Kerala, a southern Indian state.
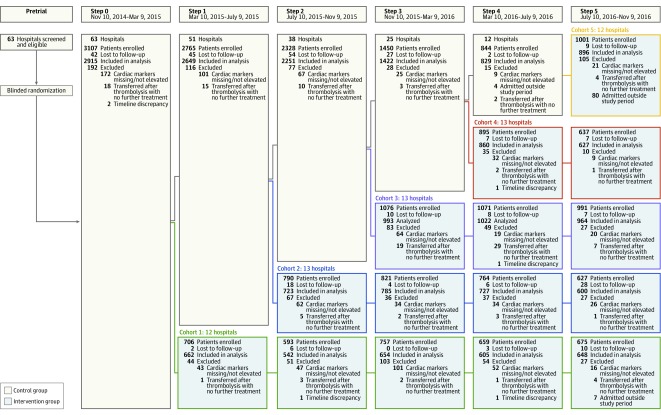
Design, setting, and participants: Cluster randomized, stepped-wedge clinical trial conducted between November 10, 2014, and November 9, 2016, in 63 hospitals in Kerala, India, with a last date of follow-up of December 31, 2016. During 5 predefined steps over the study period, hospitals were randomly selected to move in a 1-way crossover from the control group to the intervention group. Consecutively presenting patients with acute myocardial infarction were offered participation.
Interventions: Hospitals provided either usual care (control group; n = 10 066 participants [step 0: n = 2915; step 1: n = 2649; step 2: n = 2251; step 3: n = 1422; step 4; n = 829; step 5: n = 0]) or care using a quality improvement tool kit (intervention group; n = 11 308 participants [step 0: n = 0; step 1: n = 662; step 2: n = 1265; step 3: n = 2432; step 4: n = 3214; step 5: n = 3735]) that consisted of audit and feedback, checklists, patient education materials, and linkage to emergency cardiovascular care and quality improvement training.
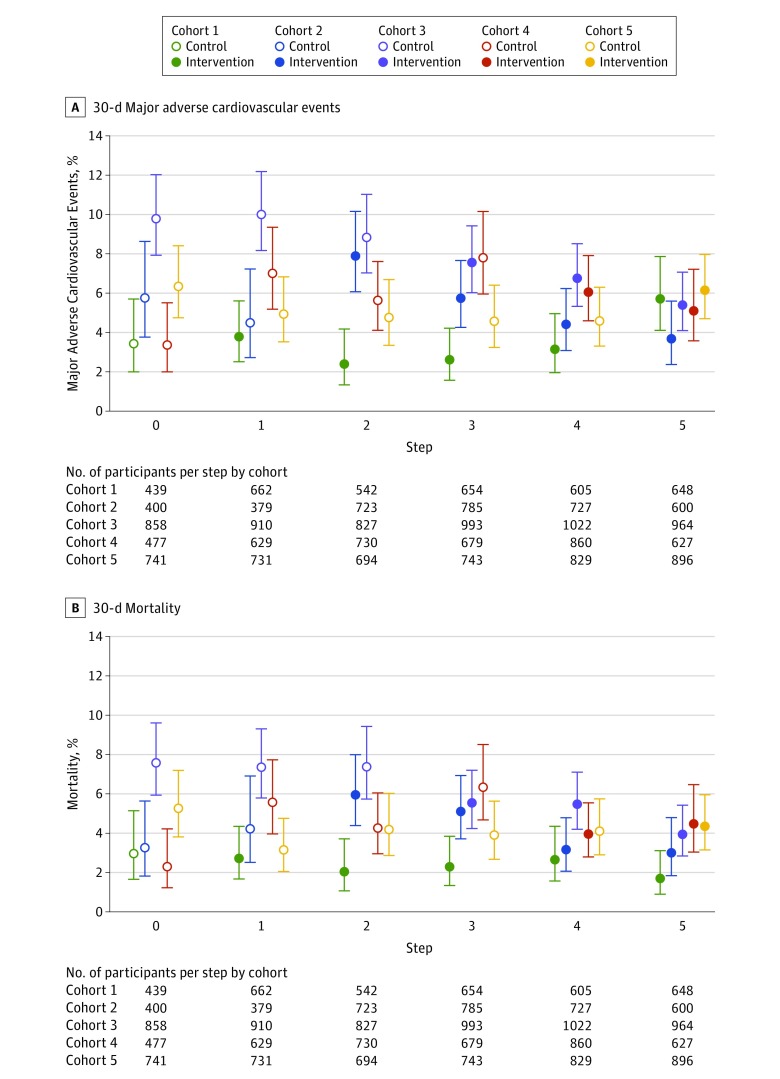
Main outcomes and measures: The primary outcome was the composite of all-cause death, reinfarction, stroke, or major bleeding using standardized definitions at 30 days. Secondary outcomes included the primary outcome's individual components, 30-day cardiovascular death, medication use, and tobacco cessation counseling. Mixed-effects logistic regression models were used to account for clustering and temporal trends.
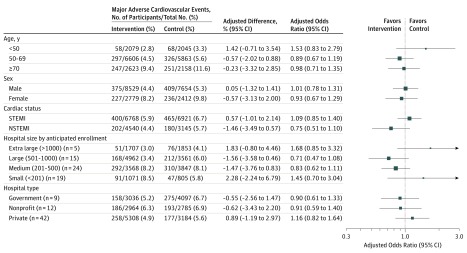
Results: Among 21 374 eligible randomized participants (mean age, 60.6 [SD, 12.0] years; n = 16 183 men [76%] ; n = 13 689 [64%] with ST-segment elevation myocardial infarction), 21 079 (99%) completed the trial. The primary composite outcome was observed in 5.3% of the intervention participants and 6.4% of the control participants. The observed difference in 30-day major adverse cardiovascular event rates between the groups was not statistically significant after adjustment (adjusted risk difference, -0.09% [95% CI, -1.32% to 1.14%]; adjusted odds ratio, 0.98 [95% CI, 0.80-1.21]). The intervention group had a higher rate of medication use including reperfusion but no effect on tobacco cessation counseling. There were no unexpected adverse events reported.
Conclusions and relevance: Among patients with acute myocardial infarction in Kerala, India, use of a quality improvement intervention compared with usual care did not decrease a composite of 30-day major adverse cardiovascular events. Further research is needed to understand the lack of efficacy.
Trial registration: clinicaltrials.gov Identifier: NCT02256657.
Conflict of interest statement
Figures
Comment in
-
Improving Evidence for Implementation of Guideline-Based Care in Low- and Middle-Income Countries.JAMA. 2018 Feb 13;319(6):554-556. doi: 10.1001/jama.2017.21905. JAMA. 2018. PMID: 29450511 No abstract available.
References
-
- Cohen MG, Fonarow GC, Peterson ED, et al. . Racial and ethnic differences in the treatment of acute myocardial infarction: findings from the Get With the Guidelines-Coronary Artery Disease program. Circulation. 2010;121(21):2294-2301. - PubMed
-
- Buckley GJ, Pittluck RE; Board on Global Health, Institute of Medicine, National Academies of Sciences, Engineering, and Medicine Improving Quality of Care in Low- and Middle-Income Countries. Washington, DC: National Academies Press; 2015. - PubMed
-
- Huffman MD, Prabhakaran D, Abraham AK, Krishnan MN, Nambiar AC, Mohanan PP; Kerala Acute Coronary Syndrome Registry Investigators . Optimal in-hospital and discharge medical therapy in acute coronary syndromes in Kerala: results from the Kerala Acute Coronary Syndrome Registry. Circ Cardiovasc Qual Outcomes. 2013;6(4):436-443. - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
