

Contrast-enhanced ultrasound (CEUS) in abdominal intervention
- PMID: 29450615
- PMCID: PMC5884902
- DOI: 10.1007/s00261-018-1473-8
Contrast-enhanced ultrasound (CEUS) in abdominal intervention
Abstract
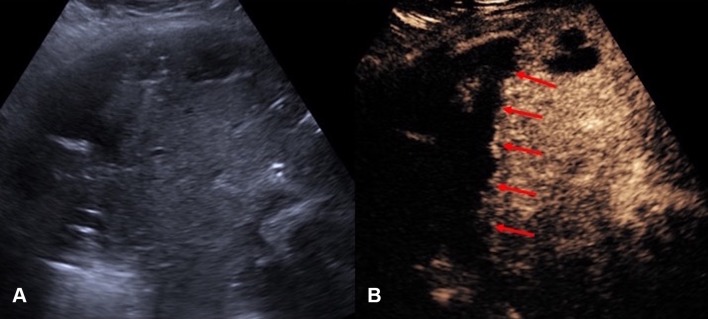
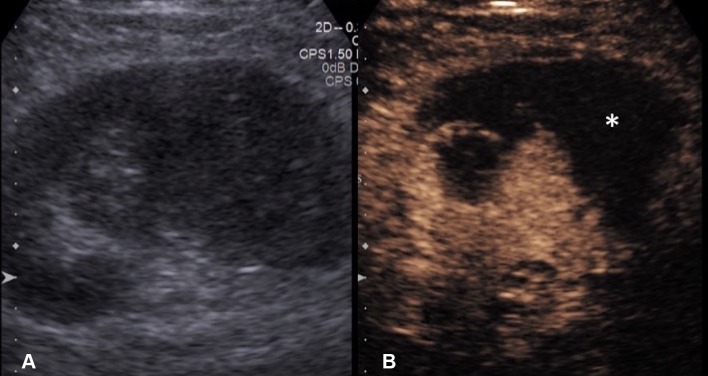
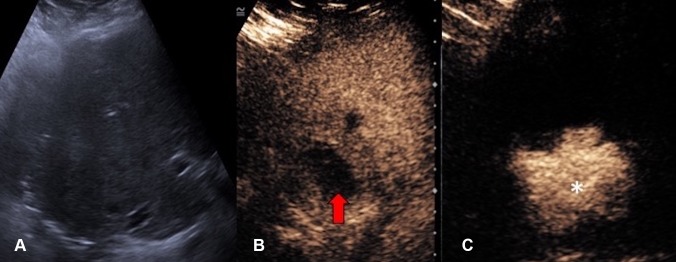
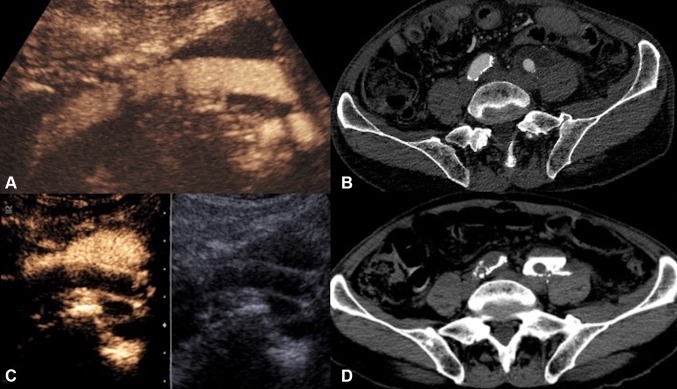
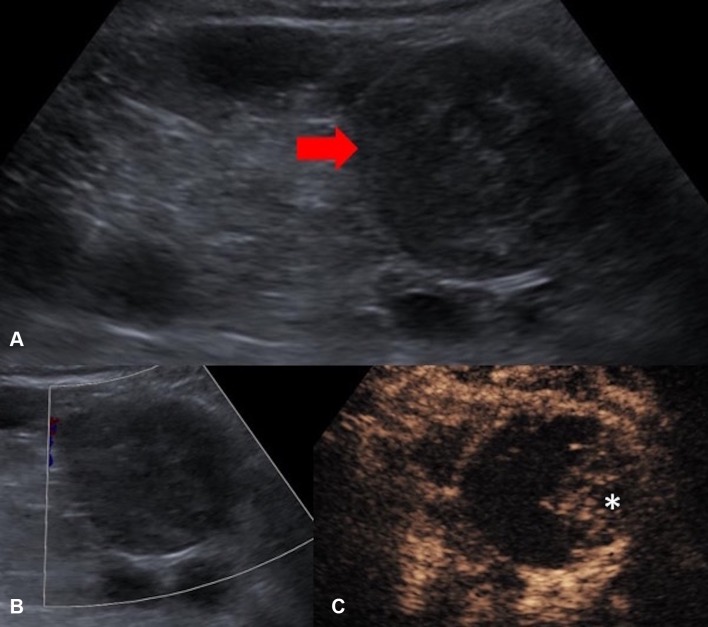
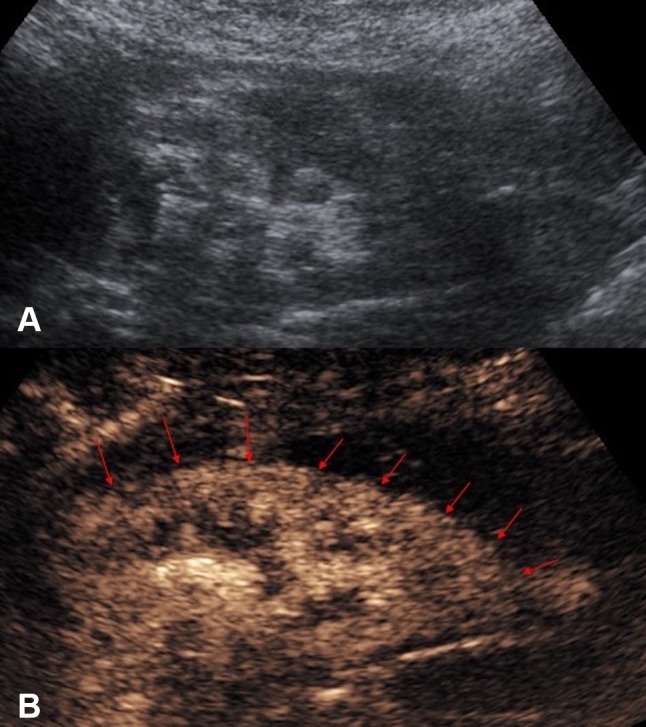
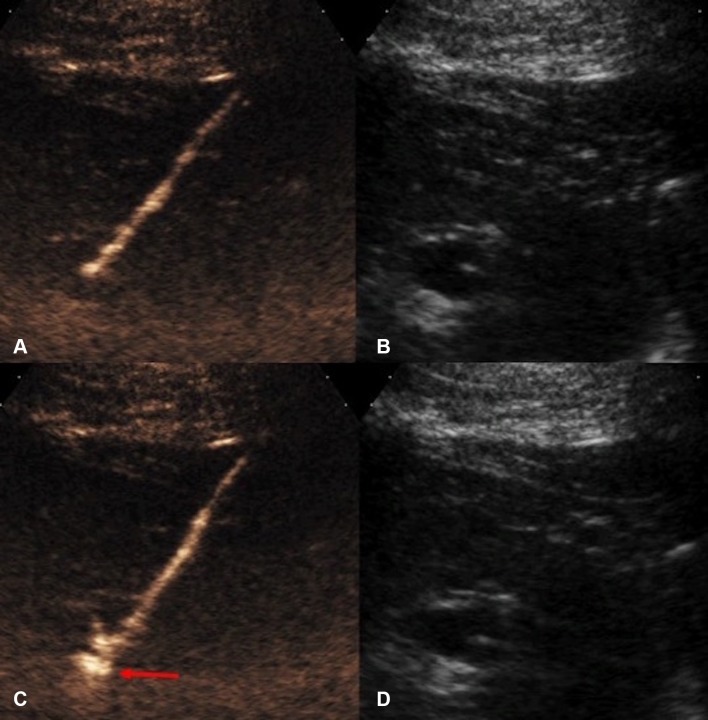
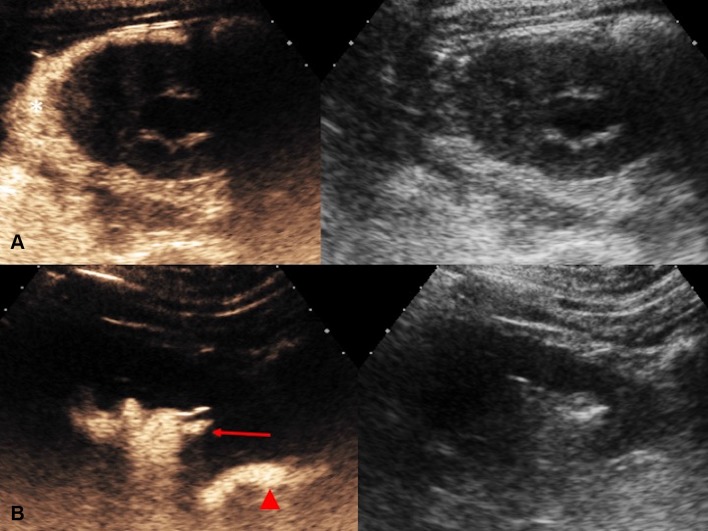
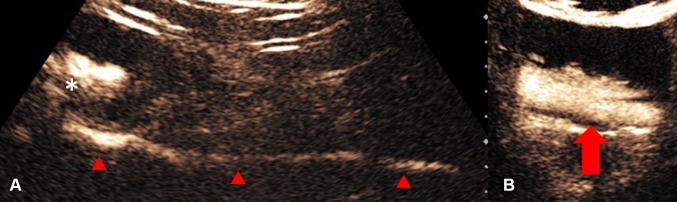
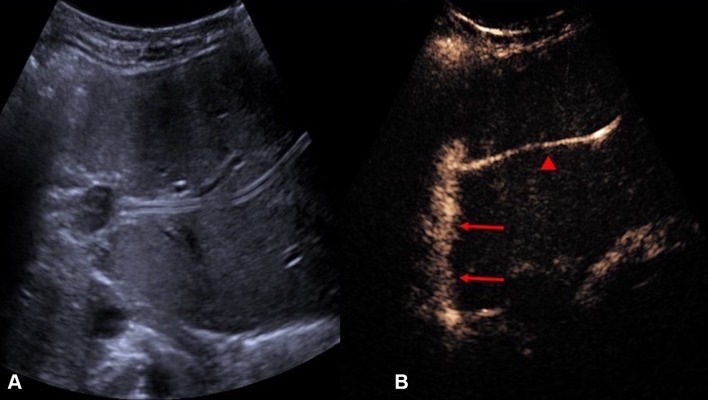
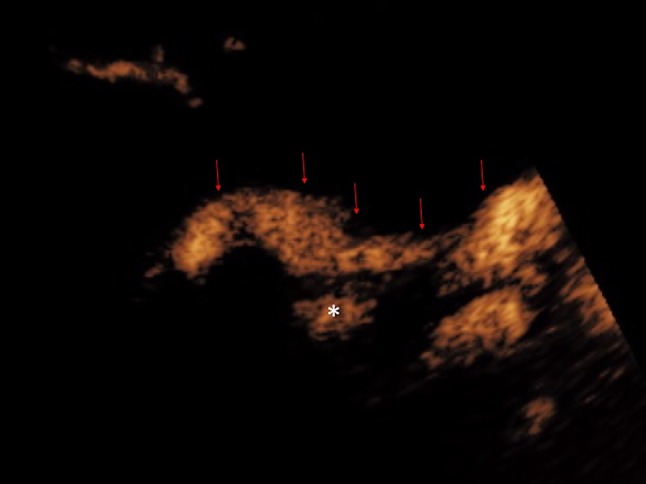
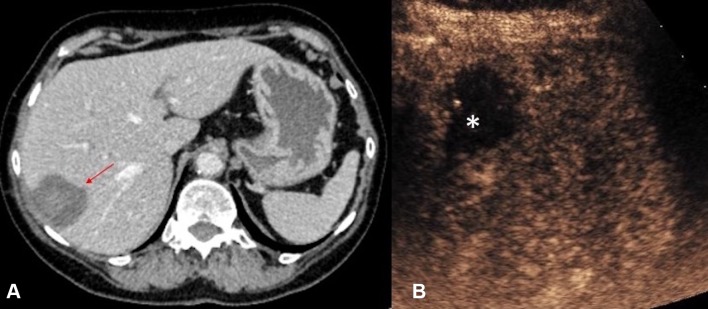
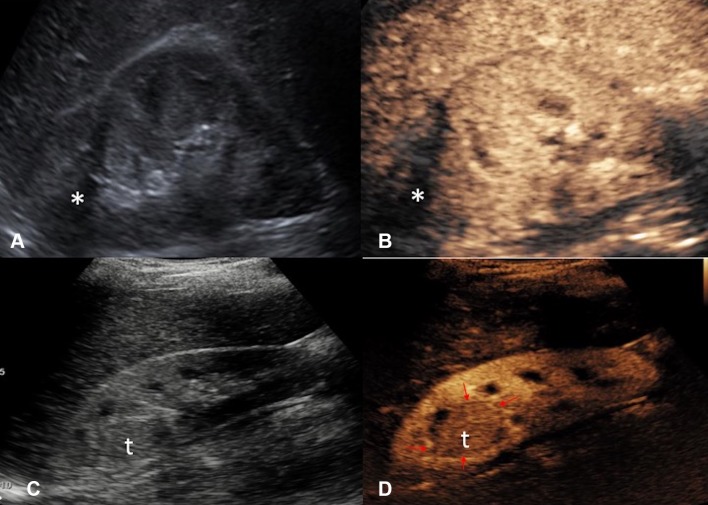
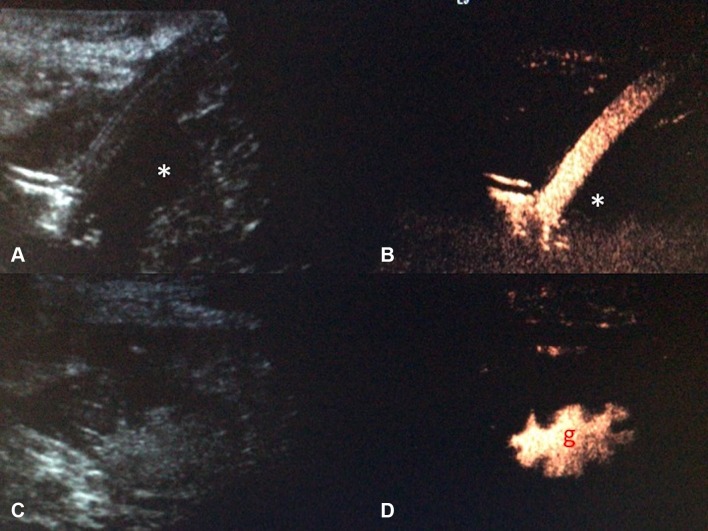
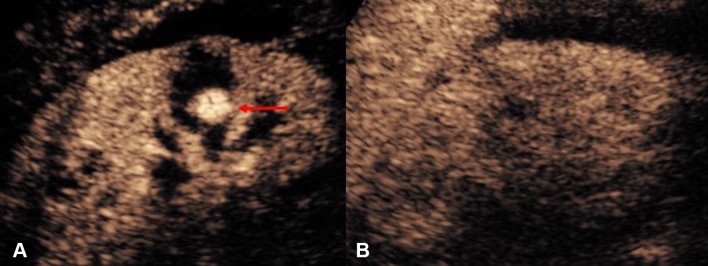
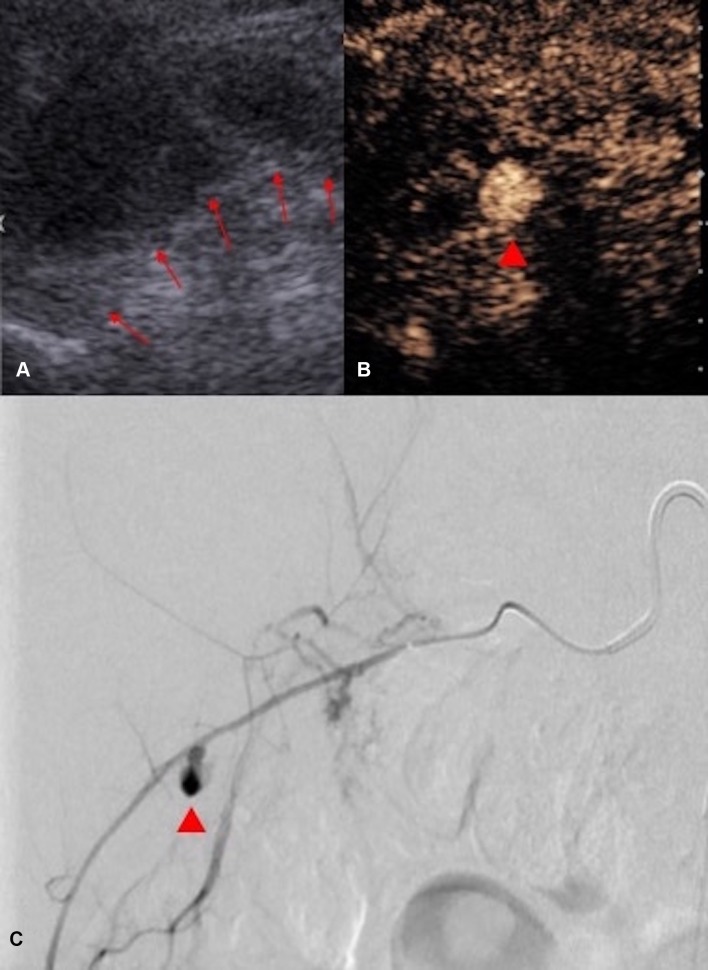
The introduction of ultrasound contrast agents has rendered contrast-enhanced ultrasound (CEUS) a valuable complementary technique to address clinically significant problems. This pictorial review describes the use of CEUS guidance in abdominal intervention and illustrates such application for a range of clinical indications. Clinical application of CEUS discussed include commonly performed abdominal interventional procedures, such as biopsy, drainage, nephrostomy, biliary intervention, abdominal tumor ablation and its subsequent monitoring, and imaging of vascular complications following abdominal intervention. The purpose of this article is to further familiarize readers with the application of CEUS, particularly its specific strength over alternative imaging modalities, in abdominal intervention.
Keywords: Abdominal intervention; Contrast enhanced ultrasound; Image guided intervention; Intervention; Interventional radiology; Ultrasound; Ultrasound contrast agents.
Conflict of interest statement
Funding
Not applicable.
Conflict of interest
MD and RR declare that they have no potential conflict of interest. GY has received lecture fees from Bracco. DH, AD and MS has received fees from Bracco for providing a training workshop on CEUS. PS has received lecture fees from Bracco, Siemens, Samsung, Philips, and Hitachi.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Figures
References
-
- Schmidbauer J, Remzi M, Memarsadeghi M, Haitel A, Klingler HC, Katzenbeisser D, Wiener H, Marberger M. Diagnostic accuracy of computed tomography-guided percutaneous biopsy of renal masses. Eur Urol. 2008;53(5):1003–1011. - PubMed
-
- Uppot RN, Harisinghani MG, Gervais DA. Imaging-guided percutaneous renal biopsy: rationale and approach. AJR Am J Roentgenol. 2010;194(6):1443–1449. - PubMed
-
- Dietrich CF, Lorentzen T, Appelbaum L, Buscarini E, Cantisani V, Correas JM, Cui XW, D’Onofrio M, Gilja OH, Hocke M, Ignee A, Jenssen C, Kabaalioglu A, Leen E, Nicolau C, Nolsoe CP, Radzina M, Serra C, Sidhu PS, Sparchez Z, Piscaglia F. EFSUMB guidelines on interventional ultrasound (INVUS), part III—abdominal treatment procedures (short version) Ultraschall Med. 2016;37(1):27–45. - PubMed
-
- Jaffe TA, Nelson RC. Image-guided percutaneous drainage: a review. Abdom Radiol (NY) 2016;41(4):629–636. - PubMed
-
- Frederick-Dyer K, Ahmad A, Arora SS, Wile G. Difficult biopsy and drainage: just say yes. Abdom Radiol (NY) 2016;41(4):706–719. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
