

Major pancreatic resections: normal postoperative findings and complications
- PMID: 29450852
- PMCID: PMC5893491
- DOI: 10.1007/s13244-018-0595-4
Major pancreatic resections: normal postoperative findings and complications
Abstract
Objectives: (1) To illustrate and describe the main types of pancreatic surgery; (2) to discuss the normal findings after pancreatic surgery; (3) to review the main complications and their radiological findings.
Background: Despite the decreased postoperative mortality, morbidity still remains high resulting in longer hospitalisations and greater costs. Imaging findings following major pancreatic resections can be broadly divided into "normal postoperative alterations" and real complications. The former should regress within a few months whereas complications may be life-threatening and should be promptly identified and treated.
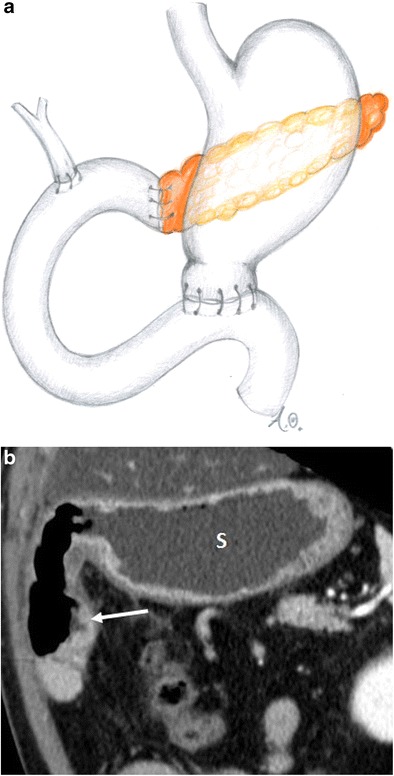
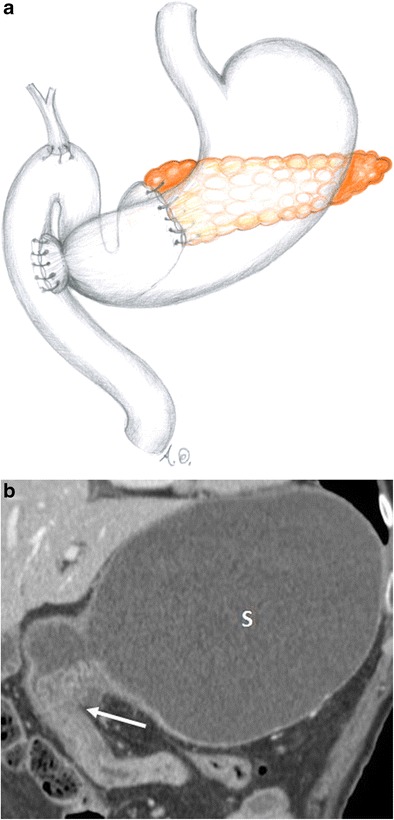
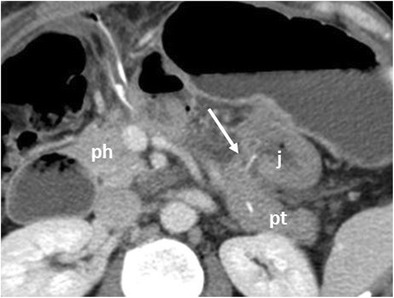
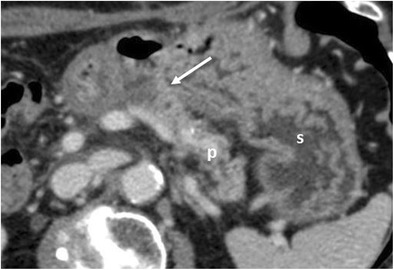
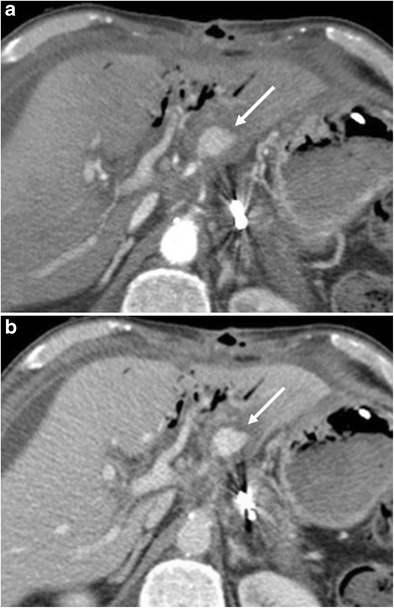
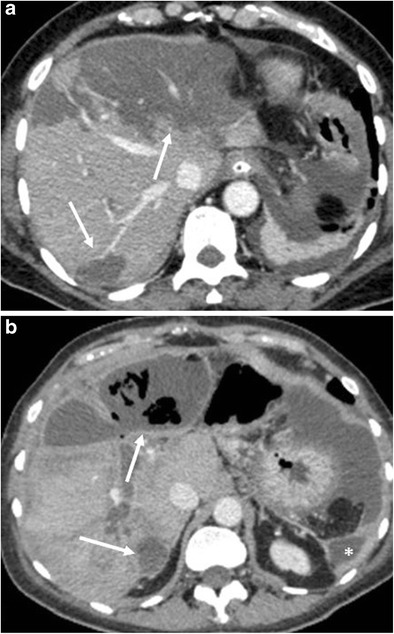
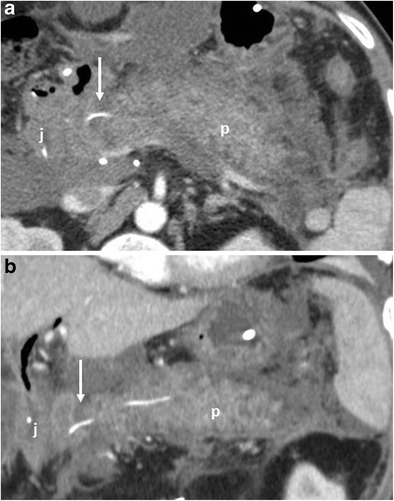
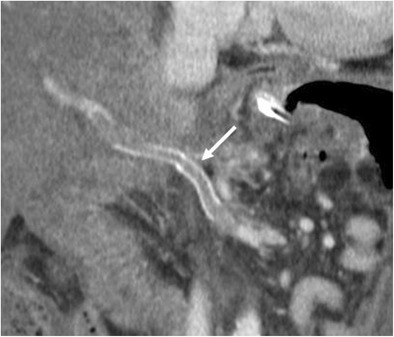
Imaging findings: CT is the most effective postoperative imaging technique. MRI and fluoroscopy are used less often and only in specific cases such as assessing the gastro-intestinal function or the biliary tree. The most common normal postoperative findings are pneumobilia, perivascular cuffing, fluid collections, lymphadenopathy, acute anastomotic oedema and stranding of the peri-pancreatic/mesenteric fat. Imaging depicts the anastomoses and the new postoperative anatomy. It can also demonstrate early and late complications: pancreatic fistula, haemorrhage, delayed gastric emptying, hepatic infarction, acute pancreatitis of the remnant, porto-mesenteric thrombosis, abscess, biliary anastomotic leaks, anastomotic stenosis and local recurrence.
Conclusions: Radiologists should be aware of surgical procedures, postoperative anatomy and normal postoperative imaging findings to better detect complications and recurrent disease.
Teaching points: • Morbidity after pancreatic resections is high. • CT is the most effective postoperative imaging technique. • Imaging depicts the anastomoses and the new postoperative anatomy. • Pancreatic fistula is the most common complication after partial pancreatic resection.
Keywords: Pancreas; Pancreatectomy; Pancreaticoduodenectomy; Pancreaticojejunostomy; Postoperative complications.
Figures









References
LinkOut - more resources
Full Text Sources
Other Literature Sources
