

Decreased early mortality associated with the treatment of acute myeloid leukemia at National Cancer Institute-designated cancer centers in California
- PMID: 29451695
- PMCID: PMC6911353
- DOI: 10.1002/cncr.31296
Decreased early mortality associated with the treatment of acute myeloid leukemia at National Cancer Institute-designated cancer centers in California
Abstract
Background: To the authors' knowledge, few population-based studies to date have evaluated the association between location of care, complications with induction therapy, and early mortality in patients with acute myeloid leukemia (AML).
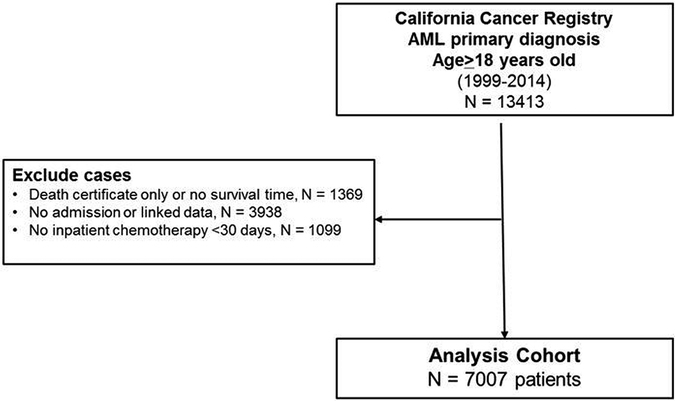
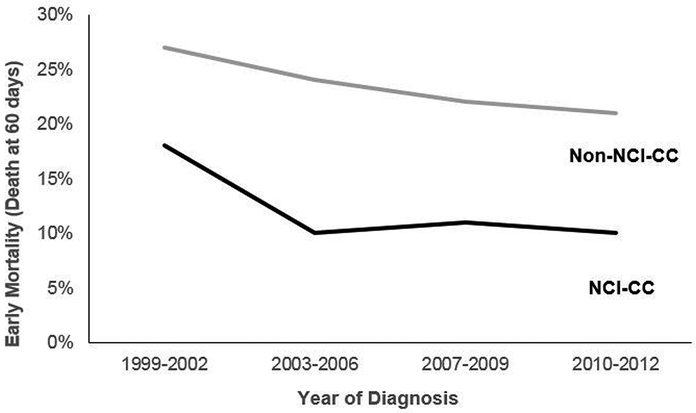
Methods: Using linked data from the California Cancer Registry and Patient Discharge Dataset (1999-2014), the authors identified adult (aged ≥18 years) patients with AML who received inpatient treatment within 30 days of diagnosis. A propensity score was created for treatment at a National Cancer Institute-designated cancer center (NCI-CC). Inverse probability-weighted, multivariable logistic regression models were used to determine associations between location of care, complications, and early mortality (death ≤60 days from diagnosis).
Results: Of the 7007 patients with AML, 1762 (25%) were treated at an NCI-CC. Patients with AML who were treated at NCI-CCs were more likely to be aged ≤65 years, live in higher socioeconomic status neighborhoods, have fewer comorbidities, and have public health insurance. Patients treated at NCI-CCs had higher rates of renal failure (23% vs 20%; P = .010) and lower rates of respiratory failure (11% vs 14%; P = .003) and cardiac arrest (1% vs 2%; P = .014). After adjustment for baseline characteristics, treatment at an NCI-CC was associated with lower early mortality (odds ratio, 0.46; 95% confidence interval, 0.38-0.57). The impact of complications on early mortality did not differ by location of care except for higher early mortality noted among patients with respiratory failure treated at non-NCI-CCs.
Conclusions: The initial treatment of adult patients with AML at NCI-CCs is associated with a 53% reduction in the odds of early mortality compared with treatment at non-NCI-CCs. Lower early mortality may result from differences in hospital or provider experience and supportive care. Cancer 2018;124:1938-45. © 2018 American Cancer Society.
Keywords: acute myeloid leukemia (AML); complications; early mortality; epidemiology; health services; location of care.
© 2018 American Cancer Society.
Conflict of interest statement
The authors have no relevant conflicts of interest to disclose.
Figures
References
-
- Deschler B, Lubbert M: Acute myeloid leukemia: epidemiology and etiology. Cancer 107:2099–107, 2006 - PubMed
-
- Ferrara F, Schiffer CA: Acute myeloid leukaemia in adults. Lancet 381:484–95, 2013 - PubMed
-
- Hahn A, Giri S, Yaghmour G, et al.: Early mortality in acute myeloid leukemia. Leuk Res 39:505–9, 2015 - PubMed
-
- Higby DJ, Cohen E, Holland JF, et al.: The prophylactic treatment of thrombocytopenic leukemic patients with platelets: a double blind study. Transfusion 14:440–6, 1974 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
