

Evaluating diagnostic indicators of urogenital Schistosoma haematobium infection in young women: A cross sectional study in rural South Africa
- PMID: 29451887
- PMCID: PMC5815575
- DOI: 10.1371/journal.pone.0191459
Evaluating diagnostic indicators of urogenital Schistosoma haematobium infection in young women: A cross sectional study in rural South Africa
Abstract
Background: Urine microscopy is the standard diagnostic method for urogenital S. haematobium infection. However, this may lead to under-diagnosis of urogenital schistosomiasis, as the disease may present itself with genital symptoms in the absence of ova in the urine. Currently there is no single reliable and affordable diagnostic method to diagnose the full spectrum of urogenital S. haematobium infection. In this study we explore the classic indicators in the diagnosis of urogenital S. haematobium infection, with focus on young women.
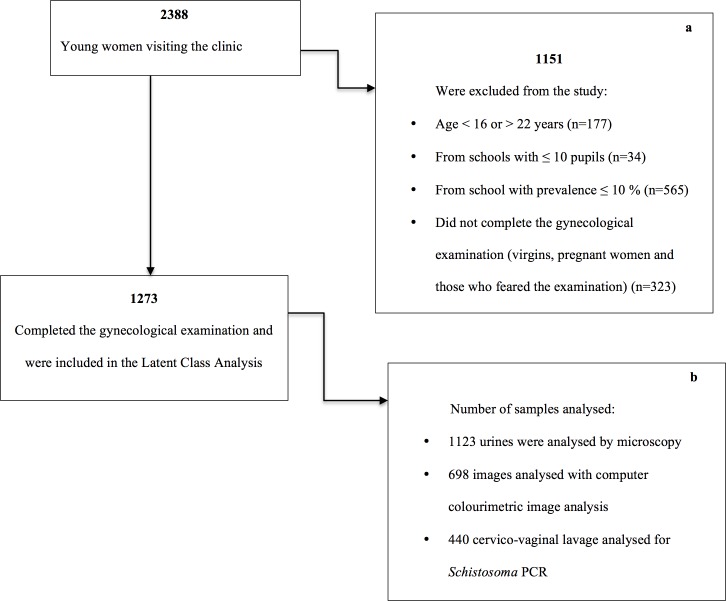
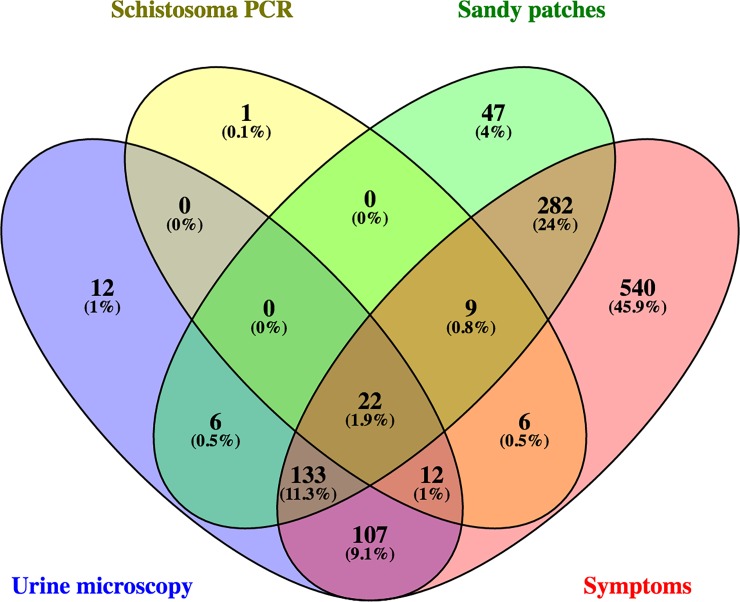
Methods: In a cross-sectional study of 1237 sexually active young women in rural South Africa, we assessed four diagnostic indicators of urogenital S. haematobium infection: microscopy of urine, polymerase chain reaction (PCR) of cervicovaginal lavage (CVL), urogenital symptoms, and sandy patches detected clinically in combination with computerised image analysis of photocolposcopic images. We estimated the accuracy of these diagnostic indicators through the following analyses: 1) cross tabulation (assumed empirical gold standard) of the tests against the combined findings of sandy patches and/or computerized image analysis and 2) a latent class model of the four indicators without assuming any gold standard.
Results: The empirical approach showed that urine microscopy had a sensitivity of 34.7% and specificity of 75.2% while the latent class analysis approach (LCA) suggested a sensitivity of 81.0% and specificity of 85.6%. The empirical approach and LCA showed that Schistosoma PCR in CVL had low sensitivity (14.1% and 52.4%, respectively) and high specificity (93.0% and 98.0, respectively). Using LCA, the presence of sandy patches showed a sensitivity of 81.6 and specificity of 42.4%. The empirical approach and LCA showed that urogenital symptoms had a high sensitivity (89.4% and 100.0%, respectively), whereas specificity was low (10.6% and 12.3%, respectively).
Conclusion: All the diagnostic indicators used in the study had limited accuracy. Using urine microscopy or Schistosoma PCR in CVL would only confirm a fraction of the sandy patches found by colposcopic examination.
Conflict of interest statement
Figures
References
-
- Kjetland EF, Ndhlovu PD, Mduluza T, Gomo E, Gwanzura L, Mason PR, et al. Simple clinical manifestations of genital Schistosoma haematobium infection in rural Zimbabwean women. Am J Trop Med Hyg. 2005;72(3):311–9. . - PubMed
-
- Utzinger J, Becker SL, van Lieshout L, van Dam GJ, Knopp S. New diagnostic tools in schistosomiasis. Clin Microbiol Infect. 2015;21(6):529–42. doi: 10.1016/j.cmi.2015.03.014 . - DOI - PubMed
-
- Poggensee G, Kiwelu I, Saria M, Richter J, Krantz I, Feldmeier H. Schistosomiasis of the lower reproductive tract without egg excretion in urine. American journal of tropical medicine and hygiene. 1998;59(5):782–3. . - PubMed
-
- Kjetland EF, Leutscher PD, Ndhlovu PD. A review of female genital schistosomiasis. Trends Parasitol. 2012;28(2):58–65. doi: 10.1016/j.pt.2011.10.008 . - DOI - PubMed
-
- Hegertun IE, Sulheim Gundersen KM, Kleppa E, Zulu SG, Gundersen SG, Taylor M, et al. S. haematobium as a common cause of genital morbidity in girls: a cross-sectional study of children in South Africa. PLoS Negl Trop Dis. 2013;7(3):e2104 doi: 10.1371/journal.pntd.0002104 ; PubMed Central PMCID: PMCPMC3605138. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
