

Impact of treatment delay on mortality in ST-segment elevation myocardial infarction (STEMI) patients presenting with and without haemodynamic instability: results from the German prospective, multicentre FITT-STEMI trial
- PMID: 29452351
- PMCID: PMC6018916
- DOI: 10.1093/eurheartj/ehy004
Impact of treatment delay on mortality in ST-segment elevation myocardial infarction (STEMI) patients presenting with and without haemodynamic instability: results from the German prospective, multicentre FITT-STEMI trial
Abstract
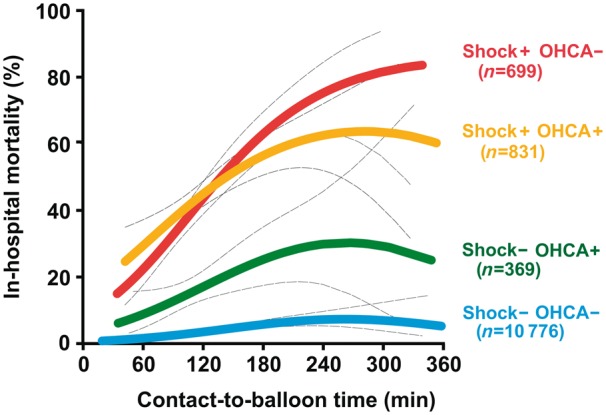
Aims: The aim of this study was to investigate the effect of contact-to-balloon time on mortality in ST-segment elevation myocardial infarction (STEMI) patients with and without haemodynamic instability.
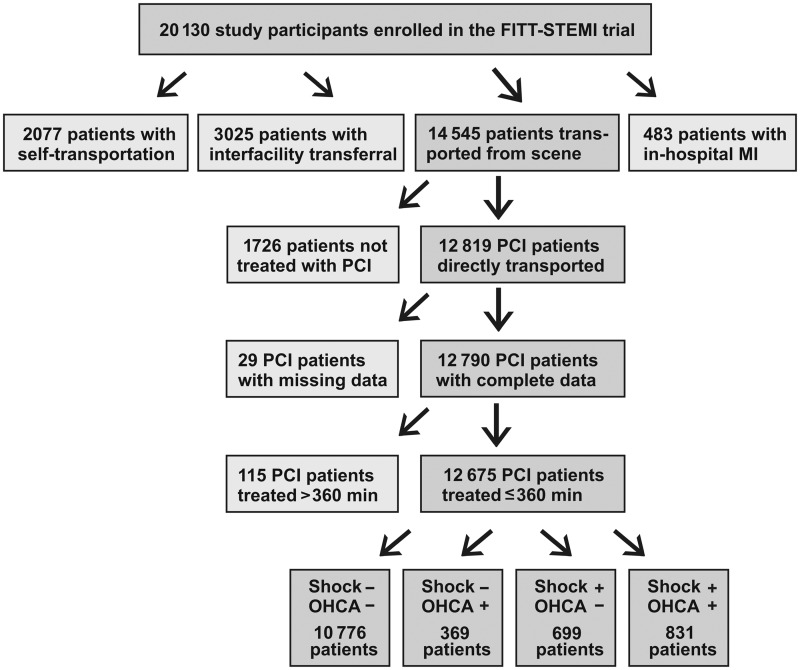
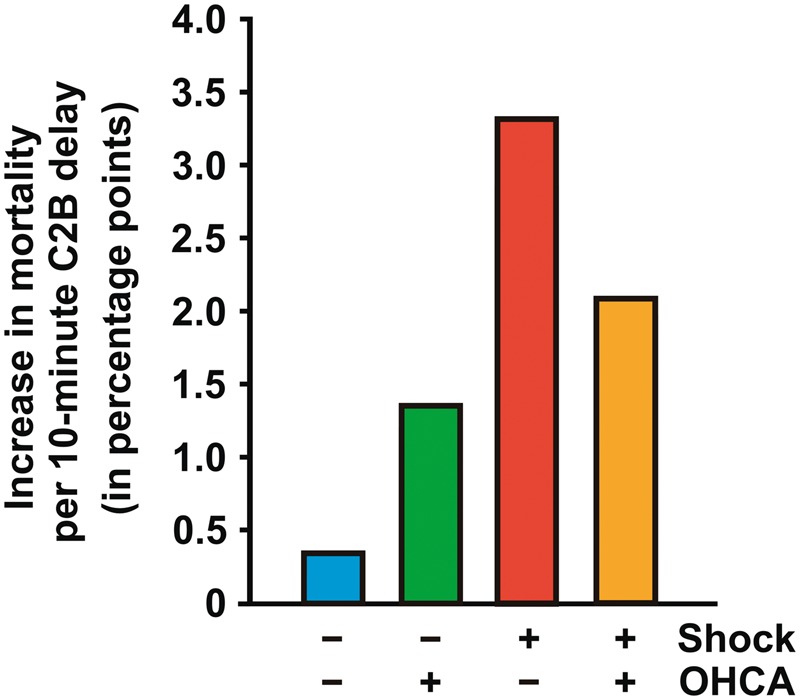
Methods and results: Using data from the prospective, multicentre Feedback Intervention and Treatment Times in ST-Elevation Myocardial Infarction (FITT-STEMI) trial, we assessed the prognostic relevance of first medical contact-to-balloon time in n = 12 675 STEMI patients who used emergency medical service transportation and were treated with primary percutaneous coronary intervention (PCI). Patients were stratified by cardiogenic shock (CS) and out-of-hospital cardiac arrest (OHCA). For patients treated within 60 to 180 min from the first medical contact, we found a nearly linear relationship between contact-to-balloon times and mortality in all four STEMI groups. In CS patients with no OHCA, every 10-min treatment delay resulted in 3.31 additional deaths in 100 PCI-treated patients. This treatment delay-related increase in mortality was significantly higher as compared to the two groups of OHCA patients with shock (2.09) and without shock (1.34), as well as to haemodynamically stable patients (0.34, P < 0.0001).
Conclusions: In patients with CS, the time elapsing from the first medical contact to primary PCI is a strong predictor of an adverse outcome. This patient group benefitted most from immediate PCI treatment, hence special efforts to shorten contact-to-balloon time should be applied in particular to these high-risk STEMI patients.
Clinical trial registration: NCT00794001.
Figures
Comment in
-
Reperfusion delay in patients with high-risk ST-segment elevation myocardial infarction: every minute counts, much more than suspected.Eur Heart J. 2018 Apr 1;39(13):1075-1077. doi: 10.1093/eurheartj/ehy069. Eur Heart J. 2018. PMID: 29452358 No abstract available.
-
[Time is life-especially in patients with acute cardiogenic shock after myocardial infarction].Med Klin Intensivmed Notfmed. 2018 Oct;113(7):577-580. doi: 10.1007/s00063-018-0450-x. Epub 2018 Jun 5. Med Klin Intensivmed Notfmed. 2018. PMID: 29869681 German. No abstract available.
-
VA-ECMO for infarct-related cardiogenic shock - Authors' reply.Lancet. 2024 Jun 8;403(10443):2487-2488. doi: 10.1016/S0140-6736(24)00964-4. Lancet. 2024. PMID: 38851286 No abstract available.
References
-
- De Luca G, Suryapranata H, Ottervanger JP, Antman EM.. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: every minute of delay counts. Circulation 2004;109:1223–1225. - PubMed
-
- Brodie BR, Webb J, Cox DA, Qureshi M, Kalynych A, Turco M, Schultheiss HP, Dulas D, Rutherford B, Antoniucci D, Stuckey T, Krucoff M, Gibbons R, Lansky A, Na Y, Mehran R, Stone GW; EMERALD Investigators. Impact of time to treatment on myocardial reperfusion and infarct size with primary percutaneous coronary intervention for acute myocardial infarction (from the EMERALD Trial). Am J Cardiol 2007;99:1680–1686. - PubMed
-
- McNamara RL, Wang Y, Herrin J, Curtis JP, Bradley EH, Magid DJ, Peterson ED, Blaney M, Frederick PD, Krumholz HM; NRMI Investigators. Effect of door-to-balloon time on mortality in patients with ST-segment elevation myocardial infarction. J Am Coll Cardiol 2006;47:2180–2186. - PubMed
-
- Brodie BR, Hansen C, Stuckey TD, Richter S, Versteeg DS, Gupta N, Downey WE, Pulsipher M.. Door-to-balloon time with primary percutaneous coronary intervention for acute myocardial infarction impacts late cardiac mortality in high-risk patients and patients presenting early after the onset of symptoms. J Am Coll Cardiol 2006;47:289–295. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
