

To what extent can behaviour change techniques be identified within an adaptable implementation package for primary care? A prospective directed content analysis
- PMID: 29452582
- PMCID: PMC5816358
- DOI: 10.1186/s13012-017-0704-7
To what extent can behaviour change techniques be identified within an adaptable implementation package for primary care? A prospective directed content analysis
Abstract
Background: Interpreting evaluations of complex interventions can be difficult without sufficient description of key intervention content. We aimed to develop an implementation package for primary care which could be delivered using typically available resources and could be adapted to target determinants of behaviour for each of four quality indicators: diabetes control, blood pressure control, anticoagulation for atrial fibrillation and risky prescribing. We describe the development and prospective verification of behaviour change techniques (BCTs) embedded within the adaptable implementation packages.
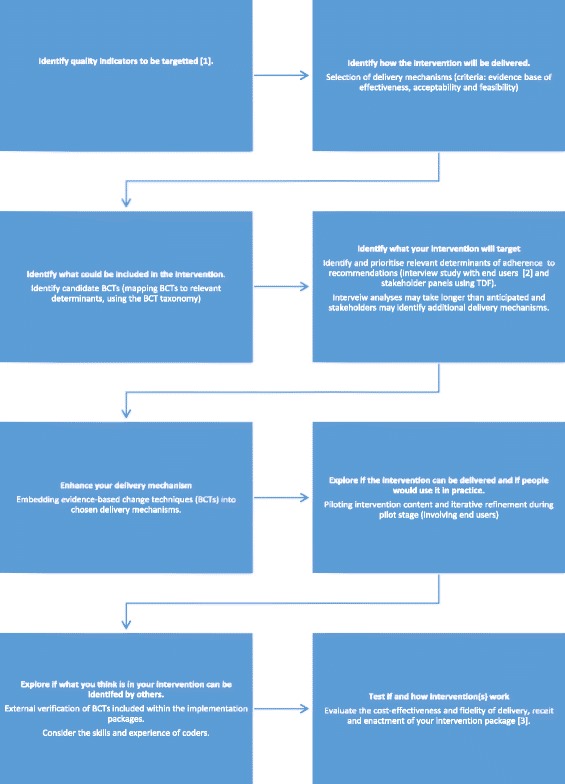
Methods: We used an over-lapping multi-staged process. We identified evidence-based, candidate delivery mechanisms-mainly audit and feedback, educational outreach and computerised prompts and reminders. We drew upon interviews with primary care professionals using the Theoretical Domains Framework to explore likely determinants of adherence to quality indicators. We linked determinants to candidate BCTs. With input from stakeholder panels, we prioritised likely determinants and intervention content prior to piloting the implementation packages. Our content analysis assessed the extent to which embedded BCTs could be identified within the packages and compared them across the delivery mechanisms and four quality indicators.
Results: Each implementation package included at least 27 out of 30 potentially applicable BCTs representing 15 of 16 BCT categories. Whilst 23 BCTs were shared across all four implementation packages (e.g. BCTs relating to feedback and comparing behaviour), some BCTs were unique to certain delivery mechanisms (e.g. 'graded tasks' and 'problem solving' for educational outreach). BCTs addressing the determinants 'environmental context' and 'social and professional roles' (e.g. 'restructuring the social and 'physical environment' and 'adding objects to the environment') were indicator specific. We found it challenging to operationalise BCTs targeting 'environmental context', 'social influences' and 'social and professional roles' within our chosen delivery mechanisms.
Conclusion: We have demonstrated a transparent process for selecting, operationalising and verifying the BCT content in implementation packages adapted to target four quality indicators in primary care. There was considerable overlap in BCTs identified across the four indicators suggesting core BCTs can be embedded and verified within delivery mechanisms commonly available to primary care. Whilst feedback reports can include a wide range of BCTs, computerised prompts can deliver BCTs at the time of decision making, and educational outreach can allow for flexibility and individual tailoring in delivery.
Keywords: Audit and feedback; Behaviour change techniques; Clinical reminders; Computerised prompts; Discriminant content analysis; Educational outreach; Implementation intervention; Theoretical Domains Framework.
Conflict of interest statement
Authors’ information
Not applicable.
Ethics approval and consent to participate
The ASPIRE programme was reviewed by the Leeds Central Research Ethics Committee in June 2012 (12/YH/0254) and National Health Service research governance permissions granted by the West Yorkshire Commissioning Support Unit.
Consent for publication
Not applicable.
Competing interests
Liz Glidewell and Robbie Foy are editors of
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Grimshaw JM, Thomas RE, Maclennan G, Fraser C, Ramsay C, Vale L, Eccles M. Effectiveness and efficiency of guideline dissemination and implementation strategies. Health Technol Assess. 2002;8:1–247. - PubMed
-
- Right Care. NHS Atlas of Variation in Healthcare. London: Public Health England; 2015.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
