

Patterns of paediatric end-of-life care: a chart review across different care settings in Switzerland
- PMID: 29452600
- PMCID: PMC5816353
- DOI: 10.1186/s12887-018-1021-2
Patterns of paediatric end-of-life care: a chart review across different care settings in Switzerland
Abstract
Background: Paediatric end-of-life care is challenging and requires a high level of professional expertise. It is important that healthcare teams have a thorough understanding of paediatric subspecialties and related knowledge of disease-specific aspects of paediatric end-of-life care. The aim of this study was to comprehensively describe, explore and compare current practices in paediatric end-of-life care in four distinct diagnostic groups across healthcare settings including all relevant levels of healthcare providers in Switzerland.
Methods: In this nationwide retrospective chart review study, data from paediatric patients who died in the years 2011 or 2012 due to a cardiac, neurological or oncological condition, or during the neonatal period were collected in 13 hospitals, two long-term institutions and 10 community-based healthcare service providers throughout Switzerland.
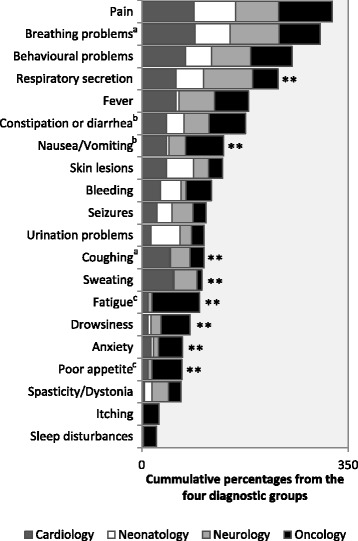
Results: Ninety-three (62%) of the 149 reviewed patients died in intensive care units, 78 (84%) of them following withdrawal of life-sustaining treatment. Reliance on invasive medical interventions was prevalent, and the use of medication was high, with a median count of 12 different drugs during the last week of life. Patients experienced an average number of 6.42 symptoms. The prevalence of various types of symptoms differed significantly among the four diagnostic groups. Overall, our study patients stayed in the hospital for a median of six days during their last four weeks of life. Seventy-two patients (48%) stayed at home for at least one day and only half of those received community-based healthcare.
Conclusions: The study provides a wide-ranging overview of current end-of-life care practices in a real-life setting of different healthcare providers. The inclusion of patients with all major diagnoses leading to disease- and prematurity-related childhood deaths, as well as comparisons across the diagnostic groups, provides additional insight and understanding for healthcare professionals. The provision of specialised palliative and end-of-life care services in Switzerland, including the capacity of community healthcare services, need to be expanded to meet the specific needs of seriously ill children and their families.
Keywords: Child; End-of-life care; Neonatology; Paediatrics; Practice patterns; Retrospective studies; Terminal care.
Conflict of interest statement
Ethics approval and consent to participate
Human Research Ethics Committees from the 11 Swiss cantons in which the study took place approved the PELICAN study (leading committee: Kantonale Ethikkommission Zürich, KEK ZH Nr. 2012-0537). Parents of eligible deceased children were informed and invited to participate in the study by the former treating team, who also acted as gatekeeper as needed. Participation was entirely voluntary and written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
