

Finger strength, individuation, and their interaction: Relationship to hand function and corticospinal tract injury after stroke
- PMID: 29453171
- PMCID: PMC5856636
- DOI: 10.1016/j.clinph.2018.01.057
Finger strength, individuation, and their interaction: Relationship to hand function and corticospinal tract injury after stroke
Abstract
Objective: The goal of this study was to determine the relative contributions of finger weakness and reduced finger individuation to reduced hand function after stroke, and their association with corticospinal tract (CST) injury.
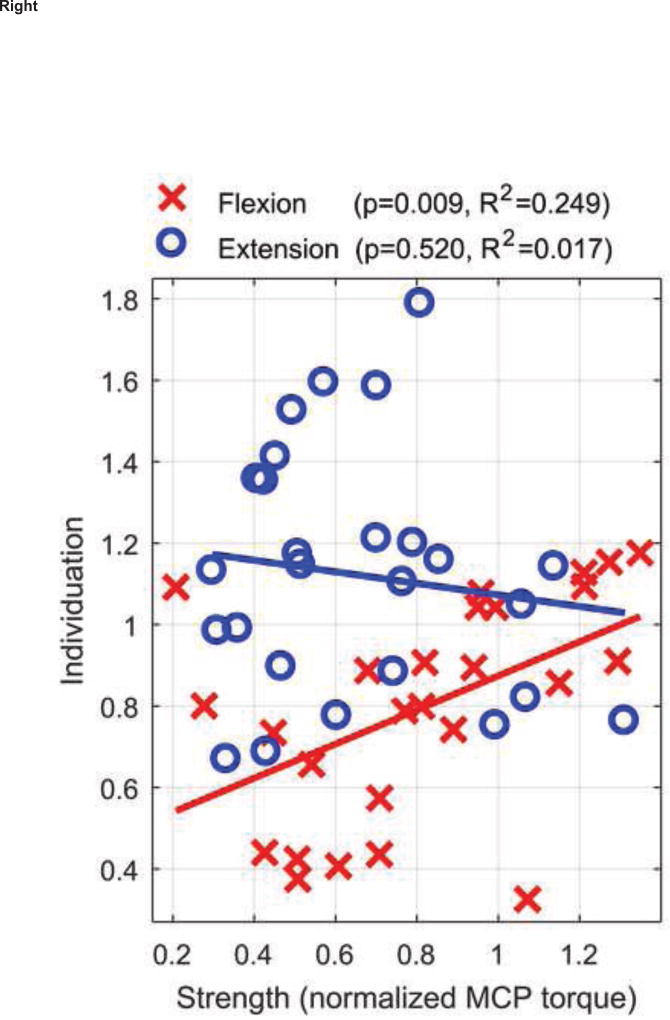
Methods: We measured individuated and synergistic maximum voluntary contractions (MVCs) of the index and middle fingers, in both flexion and extension, of 26 individuals with a chronic stroke using a robotic exoskeleton. We quantified finger strength and individuation, and defined a novel metric that combines them - "multifinger capacity". We used stepwise linear regression to identify which measure best predicted hand function (Box and Blocks Test, Nine Hole Peg Test) and arm impairment (the Upper Extremity Fugl-Meyer Test).
Results: Compared to metrics of strength or individuation, capacity survived the stepwise regression as the strongest predictor of hand function and arm impairment. Capacity was also most strongly related to presence or absence of lesion overlap with the CST.
Conclusions: Reduced strength and individuation combine to shrink the space of achievable finger torques, and it is the resulting size of this space - the multifinger capacity - that is of elevated importance for predicting loss of hand function.
Significance: Multi-finger capacity may be an important target for rehabilitative hand training.
Keywords: Corticospinal tract (CST) injury; Finger individuation; Finger strength; Hand function; Multi-finger strength; Neurorehabilitation; Stroke.
Copyright © 2018 International Federation of Clinical Neurophysiology. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
David J. Reinkensmeyer has a financial interest in Hocoma A.G. and Flint Rehabilitation Devices, LLC, companies that develop and sell rehabilitation devices. The terms of these arrangements have been reviewed and approved by the University of California, Irvine, in accordance with its conflict of interest policies. The remaining authors declare that they have no competing interests.
Figures









References
-
- Bohannon RW, Warren ME, Cogman KA. Motor variables correlated with the hand-to-mouth maneuver in stroke patients. Arch Phys Med Rehabil. 1991;72(9):682–684. - PubMed
-
- Brouwer BJ, Schryburt-Brown K. Hand function and motor cortical output poststroke: are they related? Arch Phys Med Rehabil. 2006;87(5):627–634. - PubMed
-
- Burke E, Dodakian L, See J, McKenzie A, Riley JD, Le V, Cramer SC. A multimodal approach to understanding motor impairment and disability after stroke. J Neurol. 2014;261(6):1178–1186. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
