

Sutureless Perceval Aortic Valve Versus Conventional Stented Bioprostheses: Meta-Analysis of Postoperative and Midterm Results in Isolated Aortic Valve Replacement
- PMID: 29453309
- PMCID: PMC5850177
- DOI: 10.1161/JAHA.117.006091
Sutureless Perceval Aortic Valve Versus Conventional Stented Bioprostheses: Meta-Analysis of Postoperative and Midterm Results in Isolated Aortic Valve Replacement
Abstract
Background: Aortic stenosis is the most common valvular disease and has a dismal prognosis without surgical treatment. The aim of this meta-analysis was to quantitatively assess the comparative effectiveness of the Perceval (LivaNova) valve versus conventional aortic bioprostheses.
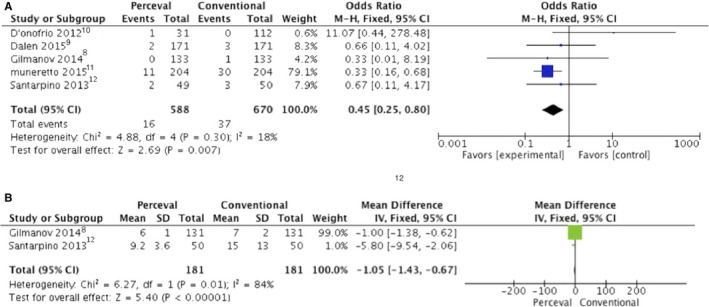
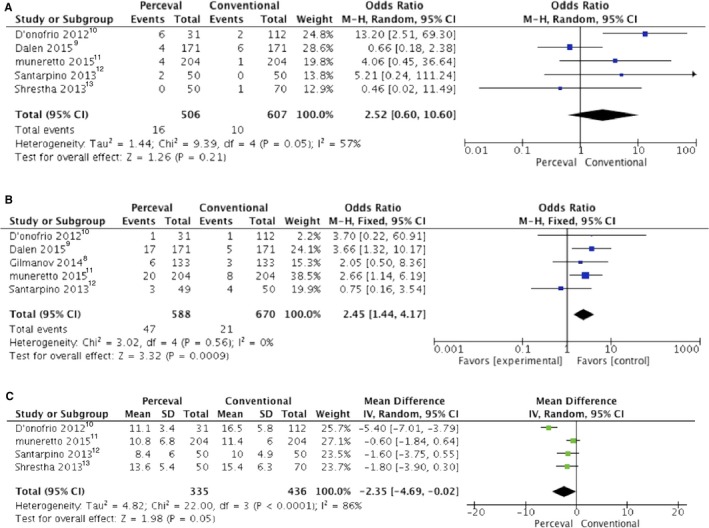
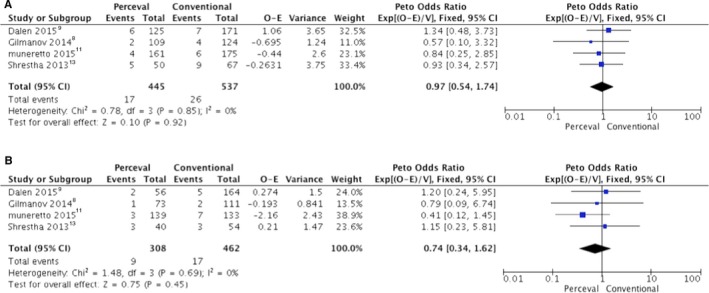
Methods and results: A total of 6 comparative studies were identified, including 639 and 760 patients who underwent, respectively, aortic valve replacement with the Perceval sutureless valve (P group) and with a conventional bioprosthesis (C group). Aortic cross-clamping and cardiopulmonary bypass duration were significantly lower in the P group. No difference in postoperative mortality was shown for the P and C groups (2.8% versus 2.7%, respectively; odds ratio [OR]: 0.99 [95% confidence interval (CI), 0.52-1.88]; P=0.98). Incidence of postoperative renal failure was lower in the P group compared with the C group (2.7% versus 5.5%; OR: 0.45 [95% CI, 0.25-0.80]; P=0.007). Incidence of stroke (2.3% versus 1.7%; OR: 1.34 [95% CI, 0.56-3.21]; P=0.51) and paravalvular leak (3.1% versus 1.6%; OR: 2.52 [95% CI, 0.60-1.06]; P=0.21) was similar, whereas P group patients received fewer blood transfusions than C group patients (1.16±1.2 versus 2.13±2.2; mean difference: 0.99 [95% CI, -1.22 to -0.75]; P=0.001). The incidence of pacemaker implantation was higher in the P than the C group (7.9% versus 3.1%; OR: 2.45 [95% CI, 1.44-4.17]; P=0.001), whereas hemodynamic Perceval performance was better (transvalvular gradient 23.42±1.73 versus 22.8±1.86; mean difference: 0.90 [95% CI, 0.62-1.18]; P=0.001), even during follow-up (10.98±5.7 versus 13.06±6.2; mean difference: -2.08 [95% CI, -3.96 to -0.21]; P=0.030). We found no difference in 1-year mortality.
Conclusions: The Perceval bioprosthesis improves the postoperative course compared with conventional bioprostheses and is an option for high-risk patients.
Keywords: Perceval valve; Sutureless bioprothesis; aortic stenosis; prosthetic heart valve.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Similar articles
-
Hemodynamic Comparison of Sutureless and Rapid-Deployment Valves with Conventional Bioprostheses.Thorac Cardiovasc Surg. 2020 Oct;68(7):584-594. doi: 10.1055/s-0039-1683426. Epub 2019 Mar 21. Thorac Cardiovasc Surg. 2020. PMID: 30900219
-
Sutureless versus Stented Bioprostheses for Aortic Valve Replacement: The Randomized PERSIST-AVR Study Design.Thorac Cardiovasc Surg. 2020 Mar;68(2):114-123. doi: 10.1055/s-0038-1675847. Epub 2018 Nov 29. Thorac Cardiovasc Surg. 2020. PMID: 30497085 Clinical Trial.
-
Sutureless versus conventional bioprostheses for aortic valve replacement in severe symptomatic aortic valve stenosis.J Thorac Cardiovasc Surg. 2021 Mar;161(3):920-932. doi: 10.1016/j.jtcvs.2020.11.162. Epub 2020 Dec 14. J Thorac Cardiovasc Surg. 2021. PMID: 33478837 Clinical Trial.
-
Aortic Stenosis and Small Aortic Annulus.Circulation. 2019 Jun 4;139(23):2685-2702. doi: 10.1161/CIRCULATIONAHA.118.038408. Epub 2019 Jun 3. Circulation. 2019. PMID: 31157994 Review.
-
A Meta-Analysis of Sutureless or Rapid-Deployment Aortic Valve Replacement.Thorac Cardiovasc Surg. 2016 Aug;64(5):400-9. doi: 10.1055/s-0035-1566130. Epub 2015 Nov 25. Thorac Cardiovasc Surg. 2016. PMID: 26606268
Cited by
-
Sevoflurane alleviates myocardial ischemia/reperfusion injury via actitation of heat shock protein-70 in patients undergoing double valve replacement surgery.Am J Transl Res. 2022 Aug 15;14(8):5529-5540. eCollection 2022. Am J Transl Res. 2022. PMID: 36105042 Free PMC article.
-
Converging rapid deployment prostheses with minimal access surgery: analysis of early outcomes.J Cardiothorac Surg. 2021 Dec 27;16(1):355. doi: 10.1186/s13019-021-01739-w. J Cardiothorac Surg. 2021. PMID: 34961528 Free PMC article.
-
ROVING PEN.Indian J Thorac Cardiovasc Surg. 2021 Sep;37(5):608-611. doi: 10.1007/s12055-021-01249-3. Epub 2021 Aug 20. Indian J Thorac Cardiovasc Surg. 2021. PMID: 34511777 Free PMC article. No abstract available.
-
Prosthetic cardiac valves: history and review of cardiac prostheses clinically available in Japan.Surg Today. 2022 Apr;52(4):521-531. doi: 10.1007/s00595-021-02361-y. Epub 2021 Aug 25. Surg Today. 2022. PMID: 34435247 Review.
-
Perceval sutureless bioprosthesis versus Trifecta sutured bioprosthesis for aortic valve replacement: immediate results of the Perfecta study.Kardiochir Torakochirurgia Pol. 2024 Sep;21(3):153-161. doi: 10.5114/kitp.2024.143499. Epub 2024 Sep 25. Kardiochir Torakochirurgia Pol. 2024. PMID: 39484109 Free PMC article.
References
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, Guyton RA, O'Gara PT, Ruiz CE, Skubas NJ, Sorajja P, Sundt TM, Thomas JD, Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Creager MA, Curtis LH, DeMets D, Guyton RA, Hochman JS, Kovacs RJ, Ohman EM, Pressler SJ, Sellke FW, Shen W‐K, Stevenson WG, Yancy CW; American College of Cardiology, American College of Cardiology/American Heart Association, American Heart Association . 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Thorac Cardiovasc Surg. 2014;148:e1–e132. - PubMed
-
- Aoyagi S, Fukunaga S, Arinaga K, Tomoeda H, Akasu K, Ueda T. Heart valve surgery in octogenarians: operative and long‐term results. Heart Vessels. 2010;25:522–528. - PubMed
-
- Bakhtiary F, Schiemann M, Dzemali O, Wittlinger T, Doss M, Ackermann H, Moritz A, Kleine P. Stentless bioprostheses improve postoperative coronary flow more than stented prostheses after valve replacement for aortic stenosis. J Thorac Cardiovasc Surg. 2006;131:883–888. - PubMed
-
- Higgins JPT, Green S, eds. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. [updated March 2011]. The Cochrane Collaboration; 2011. Available at: http://handbook.cochrane.org. Accessed December 10, 2017.
-
- Kappetein AP, Head SJ, Généreux P, Piazza N, van Mieghem NM, Blackstone EH, Brott TG, Cohen DJ, Cutlip DE, van Es G‐A, Hahn RT, Kirtane AJ, Krucoff MW, Kodali S, Mack MJ, Mehran R, Rodés‐Cabau J, Vranckx P, Webb JG, Windecker S, Serruys PW, Leon MB; Valve Academic Research Consortium‐2 . Updated standardized endpoint definitions for transcatheter aortic valve implantation: the Valve Academic Research Consortium‐2 consensus document. J Thorac Cardiovasc Surg. 2013;145:6–23. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
