

Exome sequencing has higher diagnostic yield compared to simulated disease-specific panels in children with suspected monogenic disorders
- PMID: 29453417
- PMCID: PMC5945679
- DOI: 10.1038/s41431-018-0099-1
Exome sequencing has higher diagnostic yield compared to simulated disease-specific panels in children with suspected monogenic disorders
Abstract
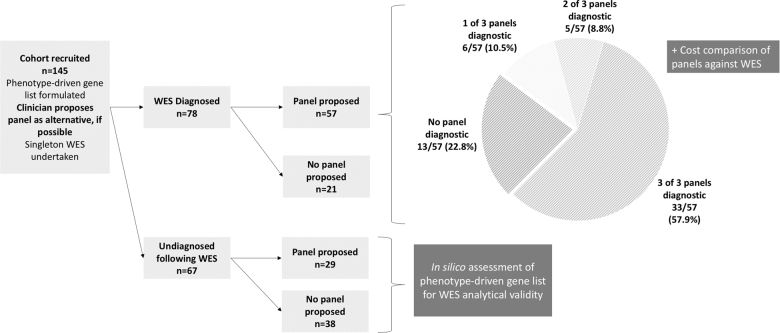
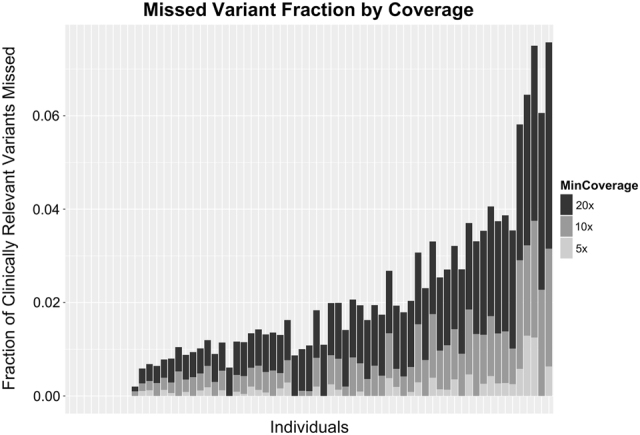
As test costs decline, whole-exome sequencing (WES) has become increasingly used for clinical diagnosis, and now represents the primary alternative to gene panel testing for patients with a suspected genetic disorder. We sought to compare the diagnostic yield of singleton-WES with simulated application of commercial gene panels in children suspected of having a genetically heterogeneous condition. Recruitment, singleton-WES and phenotype-driven variant analysis was completed for 145 paediatric patients. At recruitment, clinicians were required to propose commercial gene panel tests as an alternative to WES and nominate a phenotype-driven candidate gene list. In WES-diagnosed children, three commercial options for each proposed panel were identified and evaluated for hypothetical diagnostic yield assuming 100% analytical sensitivity and specificity. We compared the price of WES with the least costly panel in WES-diagnosed children. In WES-undiagnosed children, we evaluated the exonic coverage of their phenotype-driven gene list using aggregate data. WES diagnoses were made in genes not included in at least one-of-three commercial panels in 42% of cases. Had a panel been selected instead, 23% of WES-diagnosed children would not have been diagnosed. In 26% of cases, the least costly panel option would have been more expensive than WES. Evaluation of WES coverage found that at the most stringent level of 20× coverage, the likelihood of missing a clinically relevant variant in a candidate gene list was maximally 8%. The broader coverage of WES makes it a superior alternative to gene panel testing at similar financial cost for children with suspected complex monogenic phenotypes.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
