

Low Serum IgE Is a Sensitive and Specific Marker for Common Variable Immunodeficiency (CVID)
- PMID: 29453744
- PMCID: PMC5934300
- DOI: 10.1007/s10875-018-0476-0
Low Serum IgE Is a Sensitive and Specific Marker for Common Variable Immunodeficiency (CVID)
Abstract
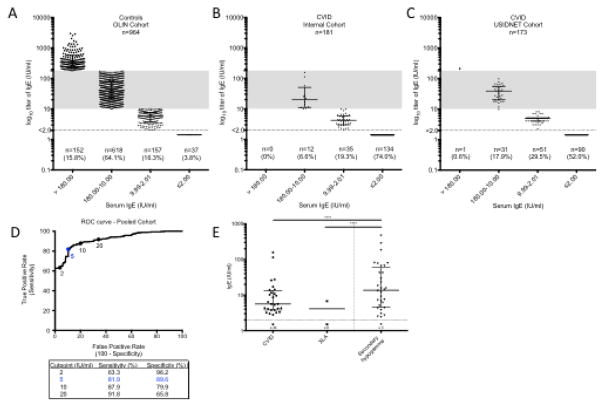
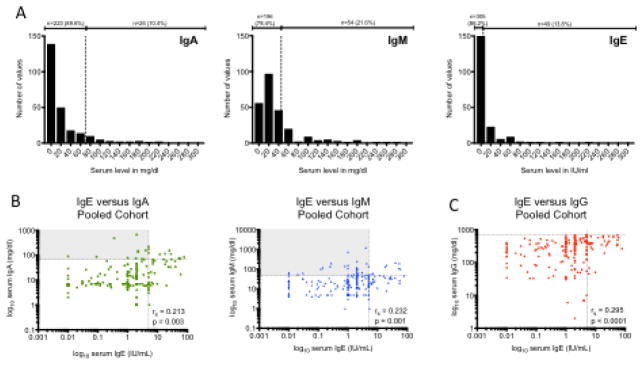
Although small prior studies have suggested that IgE can be low in common variable immunodeficiency (CVID), the workup for patients with recurrent infections and suspected hypogammaglobulinemia does not include the routine measurement of serum IgE. We sought to test the hypothesis that low/undetectable serum IgE is characteristic of CVID by comparing the frequency of low/undetectable serum IgE in healthy controls and patients with CVID. We measured total serum IgE in a large multi-center cohort of patients with CVID (n = 354) and compared this to large population-based cohorts of children and adults. We further compared IgE levels in patients with CVID to those with other forms of humoral immunodeficiency, and in a subset, measured levels of allergen-specific serum IgE and IgG subclasses. Lastly, we evaluated for the presence of IgE in commercially available immunoglobulin replacement therapy (IgRT) products. An undetectable serum IgE (< 2 IU/ml) occurs in only 3.3% (95% CI, 1.9-5.7%) of the general population. In contrast, an undetectable IgE occurs in 75.6% (95% CI, 65.6-85.7%) of patients with CVID. Conversely, a high IgE (> 180 IU/ml) is very uncommon in CVID (0.3% of patients). IgE is > 2 IU/ml in 91.2% of patients with secondary hypogammaglobulinemia, and thus, an IgE < LLOD is suggestive of a primary humoral immunodeficiency. Allergen-specific IgE is not detectable in 96.5% of patients with CVID. Sufficient quantities of IgE to change the total serum IgE are not contained in IgRT. The IgG1/IgG4 ratio is increased in subjects with low IgE, regardless of whether they are controls or have CVID. These findings support the routine measurement of serum IgE in the workup of patients with hypogammaglobulinemia.
Keywords: Common variable immunodeficiency; IgE; IgE deficiency; secondary hypogammaglobulinemia.
Conflict of interest statement
John Routes received independent contractor fees from CSL Behring. The rest of the authors declare that they have no relevant conflicts of interest.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
