

24 vs. 72 hours of hypothermia for pediatric cardiac arrest: A pilot, randomized controlled trial
- PMID: 29454009
- PMCID: PMC5899619
- DOI: 10.1016/j.resuscitation.2018.02.008
24 vs. 72 hours of hypothermia for pediatric cardiac arrest: A pilot, randomized controlled trial
Abstract
Aim: Children surviving cardiac arrest (CA) lack proven neuroprotective therapies. The role of biomarkers in assessing response to interventions is unknown. We hypothesized that 72 versus 24 h of hypothermia (HT) would produce more favorable biomarker profiles after pediatric CA.
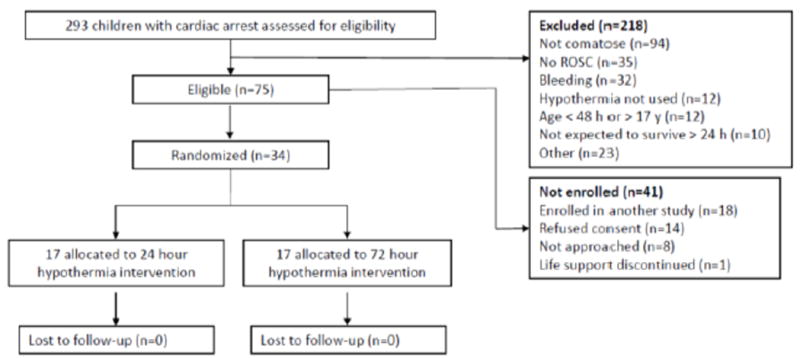
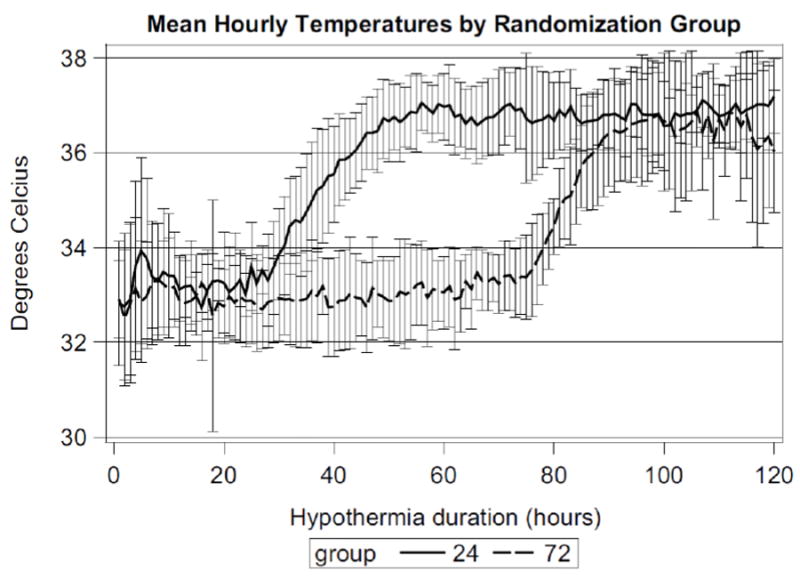
Methods: This single center pilot randomized trial tested HT (33 ± 1 °C) for 24 vs. 72 h in 34 children with CA. Children comatose after return of circulation aged 1 week to 17 years and treated with HT by their physician were eligible. Serum was collected twice daily on days 1-4 and once on day 7. Mortality was assessed at 6 months.
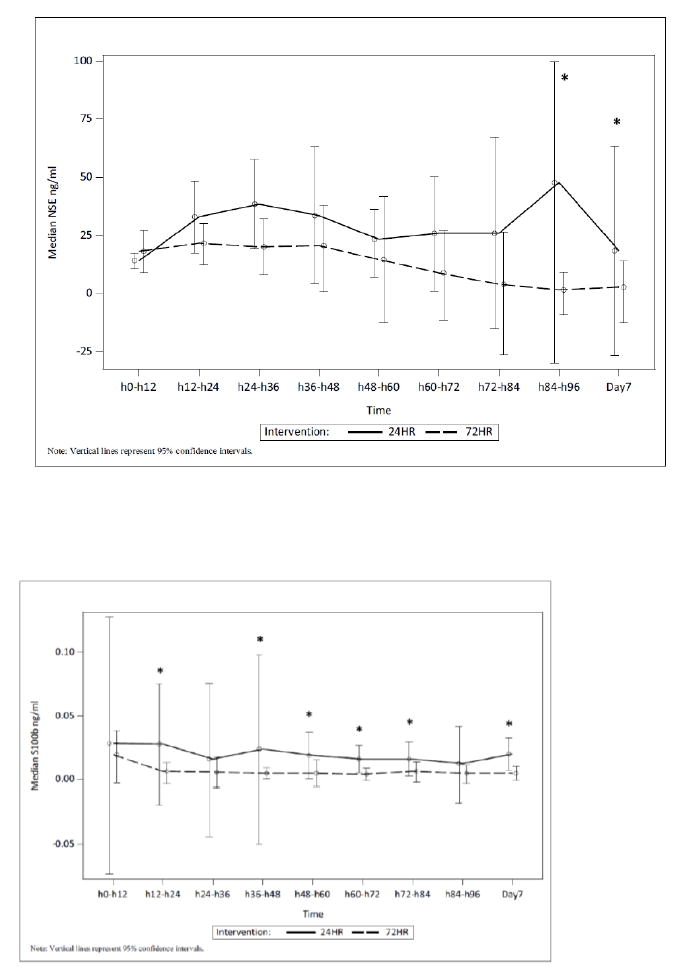
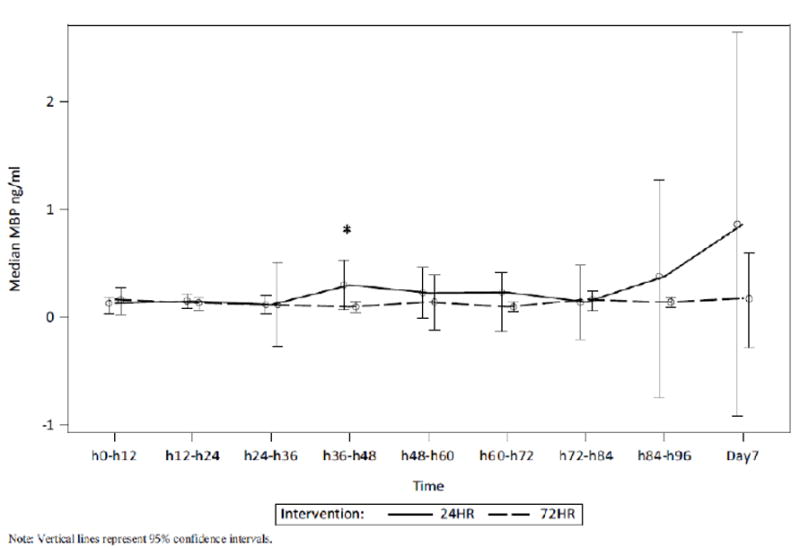
Results: Patient characteristics, baseline biomarker concentrations, and adverse events were similar between groups. Eight (47%) and 4 (24%) children died in the 24 h and 72 h groups, p = .3. Serum neuron specific enolase (NSE) concentration was increased in the 24 vs. 72 h group at 84 h-96 h (median [interquartile range] 47.7 [3.9, 79.9] vs. 1.4 [0.0, 11.1] ng/ml, p = .02) and on day 7 (18.2 [3.2, 74.0] vs. 2.6 [0.0, 12.8] ng/ml, p = .047). Serum S100b was increased in the 24 h vs. 72 h group at 12 h-24 h, 36 h-84 h, and on day 7, all p < 0.05. HT duration was associated with S100b (but not NSE or MBP) concentration on day 7 in multivariate analyses.
Conclusion: Serum biomarkers show promise as theragnostic tools in pediatric CA. Our biomarker and safety data also suggest that 72 h duration after pediatric CA warrants additional exploration.
Keywords: Biomarker; Cardiac arrest; Critical care; Neurologic disorders; Outcome; Pediatric.
Copyright © 2018 Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Serum biomarkers of brain injury to classify outcome after pediatric cardiac arrest*.Crit Care Med. 2014 Mar;42(3):664-74. doi: 10.1097/01.ccm.0000435668.53188.80. Crit Care Med. 2014. PMID: 24164954 Free PMC article.
-
Neuron-specific enolase and S-100b in prolonged targeted temperature management after cardiac arrest: A randomised study.Resuscitation. 2018 Jan;122:79-86. doi: 10.1016/j.resuscitation.2017.11.052. Epub 2017 Nov 22. Resuscitation. 2018. PMID: 29175384 Clinical Trial.
-
The biomarkers neuron-specific enolase and S100b measured the day following admission for severe accidental hypothermia have high predictive values for poor outcome.Resuscitation. 2017 Dec;121:49-53. doi: 10.1016/j.resuscitation.2017.10.006. Epub 2017 Oct 7. Resuscitation. 2017. PMID: 29017847
-
Combining NSE and S100B with clinical examination findings to predict survival after resuscitation from cardiac arrest.Resuscitation. 2014 Aug;85(8):1025-9. doi: 10.1016/j.resuscitation.2014.04.020. Epub 2014 Apr 30. Resuscitation. 2014. PMID: 24795283 Free PMC article.
-
Prognostic utility of neuroinjury biomarkers in post out-of-hospital cardiac arrest (OHCA) patient management.Med Hypotheses. 2017 Aug;105:34-47. doi: 10.1016/j.mehy.2017.06.016. Epub 2017 Jun 24. Med Hypotheses. 2017. PMID: 28735650 Review.
Cited by
-
The current temperature: A survey of post-resuscitation care across Australian and New Zealand intensive care units.Resusc Plus. 2020 May 21;1-2:100002. doi: 10.1016/j.resplu.2020.100002. eCollection 2020 Mar-Jun. Resusc Plus. 2020. PMID: 34223289 Free PMC article.
-
Personalising Outcomes after Child Cardiac Arrest (POCCA): design and recruitment challenges of a multicentre, observational study.BMJ Open. 2020 Oct 27;10(10):e039323. doi: 10.1136/bmjopen-2020-039323. BMJ Open. 2020. PMID: 33109667 Free PMC article.
-
The Utility of a Point-of-Care Transcranial Doppler Ultrasound Management Algorithm on Outcomes in Pediatric Asphyxial Out-of-Hospital Cardiac Arrest - An Exploratory Investigation.Front Med (Lausanne). 2022 Jan 28;8:690405. doi: 10.3389/fmed.2021.690405. eCollection 2021. Front Med (Lausanne). 2022. PMID: 35155456 Free PMC article.
-
The Effect of Therapeutic Hypothermia on Ischemic Brain Injury in a Rat Model of Cardiac Arrest: An Assessment Using 18F-FDG PET.Diagnostics (Basel). 2024 Aug 2;14(15):1674. doi: 10.3390/diagnostics14151674. Diagnostics (Basel). 2024. PMID: 39125550 Free PMC article.
-
The Effect of Therapeutic Hypothermia after Cardiac Arrest on the Neurological Outcome and Survival-A Systematic Review of RCTs Published between 2016 and 2020.Int J Environ Res Public Health. 2021 Nov 11;18(22):11817. doi: 10.3390/ijerph182211817. Int J Environ Res Public Health. 2021. PMID: 34831572 Free PMC article.
References
-
- Kuisma M, Suominen P, Korpela R. Paediatric out-of-hospital cardiac arrests--epidemiology and outcome. Resuscitation. 1995;30(2):141–150. - PubMed
-
- Reis AG, Nadkarni V, Perondi MB, Grisi S, Berg RA. A prospective investigation into the epidemiology of in-hospital pediatric cardiopulmonary resuscitation using the international Utstein reporting style. Pediatrics. 2002;109(2):200–209. - PubMed
-
- Young KD, Gausche-Hill M, McClung CD, Lewis RJ. A prospective, population-based study of the epidemiology and outcome of out-of-hospital pediatric cardiopulmonary arrest. Pediatrics. 2004;114(1):157–164. - PubMed
-
- Nadkarni VM, Larkin GL, Peberdy MA, et al. First documented rhythm and clinical outcome from inhospital cardiac arrest among children and adults. JAMA. 2006;295(1):50–57. - PubMed
-
- de Mos N, van Litsenburg RR, McCrindle B, Bohn DJ, Parshuram CS. Pediatric in-intensive-care-unit cardiac arrest: incidence, survival, and predictive factors. Crit Care Med. 2006;34(4):1209–1215. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
