

Quality of life, satisfaction and outcomes after ministernotomy versus full sternotomy isolated aortic valve replacement (QUALITY-AVR): study protocol for a randomised controlled trial
- PMID: 29454380
- PMCID: PMC5816540
- DOI: 10.1186/s13063-018-2486-x
Quality of life, satisfaction and outcomes after ministernotomy versus full sternotomy isolated aortic valve replacement (QUALITY-AVR): study protocol for a randomised controlled trial
Abstract
Background: During the last decade, the use of ministernotomy in cardiac surgery has increased. Quality of life and patient satisfaction after ministernotomy have never been compared to conventional full sternotomy in randomised trials. The aim of the study is to determine if this minimally invasive approach improves quality of life, satisfaction and clinical morbimortality outcomes.
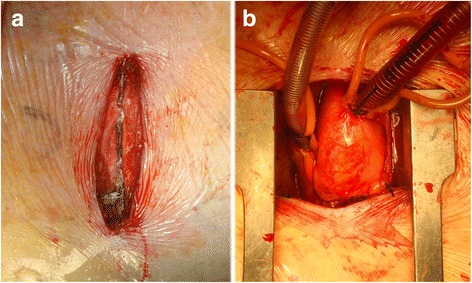
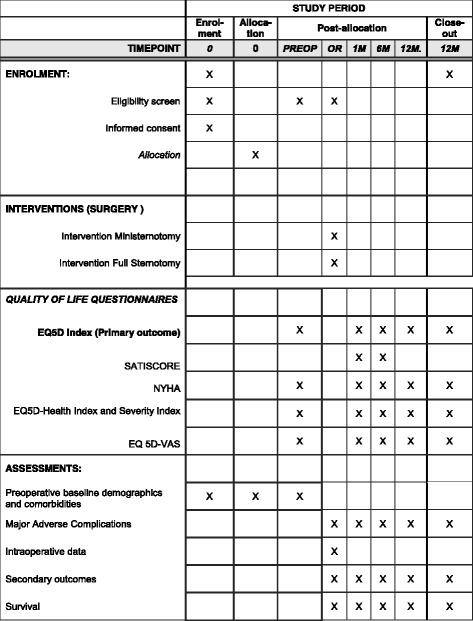
Methods/design: The QUALITY-AVR trial is a single-blind, single-centre, independent, and pragmatic randomised clinical trial comparing ministernotomy ("J" shaped upper hemisternotomy toward right 4th intercostal space) to full sternotomy in patients with isolated severe aortic stenosis scheduled for elective aortic valve replacement. One hundred patients will be randomised in a 1:1 computational fashion. Sample size was determined for the primary end point with alpha error of 0.05 and with power of 90% in detecting differences between intervention groups of ≥ 0.10 points in change from baseline quality of life Questionnaire EuroQOL-index (EQ-5D-5 L®), measured at 1, 6 or 12 months. Secondary endpoints are: the differences in change from other baseline EQ-5D-5 L® utilities (visual analogue scale, Health Index and Severity Index), cardiac surgery specific satisfaction questionnaire (SATISCORE®), a combined safety endpoint of four major adverse complications at 1 month (all-cause mortality, acute myocardial infarction, neurologic events and acute renal failure), bleeding through drains within the first 24 h, intubation time, postoperative hospital and intensive care unit length of stay, transfusion needs during the first 72 h and 1-year survival rates. Clinical follow up is scheduled at baseline, 1, 6, and 12 months after randomization. All clinical outcomes are recorded following the Valve Academic Research Consortium 2 criteria.
Discussion: The QUALITY-AVR trial aims to test the hypothesis that ministernotomy improves quality of life, satisfaction and clinical outcomes in patients referred for isolated aortic valve replacement. Statistically significant differences favouring ministernotomy could modify the surgical "gold standard" for aortic stenosis surgery, and subsequently the need to change the control group in transcatheter aortic valve implantation trials. Recruitment started on 18 March 2016. In November 2017, 75 patients were enrolled.
Trial registration: ClinicalTrials.gov , NCT02726087 . Registered on 13 March 2016.
Keywords: Aortic stenosis; Aortic valve replacement; Clinical trials; Ministernotomy; Quality of life; Satisfaction.
Conflict of interest statement
Ethics approval and consent to participate
This trial has been approved by our Institution’s Ethics Committee for Research (CEI Provincial de Málaga, Institutional Review Board), and was registered at
Consent for publication
Figure 1 was ceded with permission by Edwards Lifesciences®.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Bonow JM, O’Brien SM, Wu C, Sikora JA, Griffith BP, Gammie JS. Isolated aortic valve replacement in North America comprising 108,687 patients in 10 years: changes in risks, valve types, and outcomes in the STS National Database. J Thorac Cardiovasc Surg. 2009;137:82–90. doi: 10.1016/j.jtcvs.2008.08.015. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
