

Simplified percutaneous closure of patent foramen ovale and atrial septal defect with use of plain fluoroscopy: Single operator experience in 110 consecutive patients
- PMID: 29455783
- PMCID: PMC5902918
- DOI: 10.1016/j.ihj.2017.07.020
Simplified percutaneous closure of patent foramen ovale and atrial septal defect with use of plain fluoroscopy: Single operator experience in 110 consecutive patients
Abstract
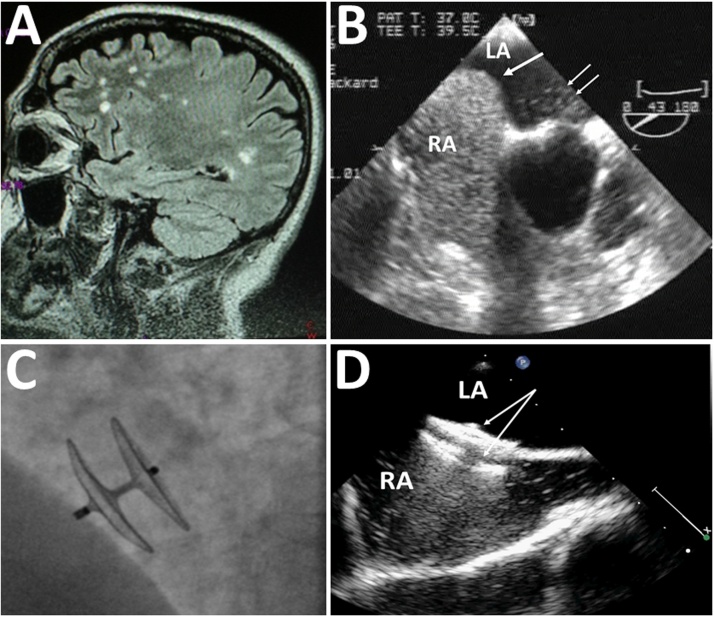
Objective: Percutaneous closure of patent foramen ovale (PFO) and atrial septal defect (ASD) is routinely performed under general anesthesia or deep sedation and use of transesophageal (TEE) or intracardiac echocardiography, incurring longer duration and higher cost. We have used a simplified, economical, fluoroscopy-only guided approach with local anesthesia, and herein report our data.
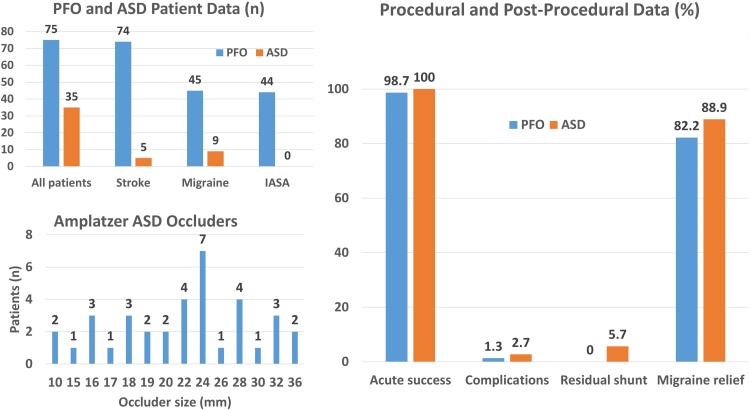
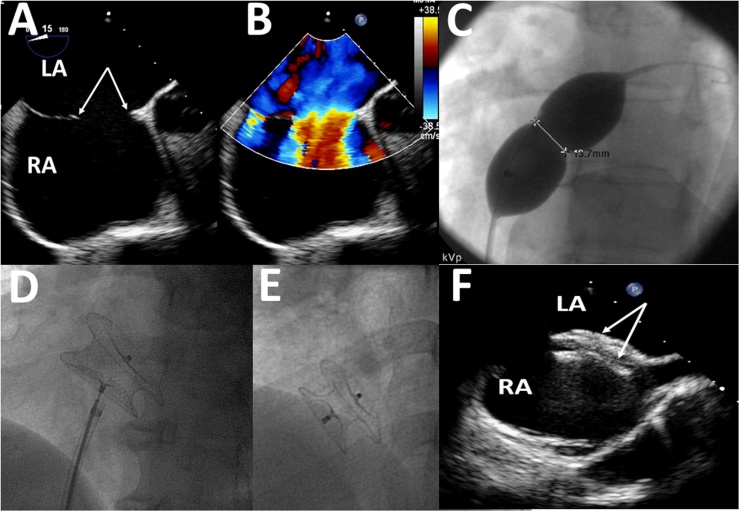
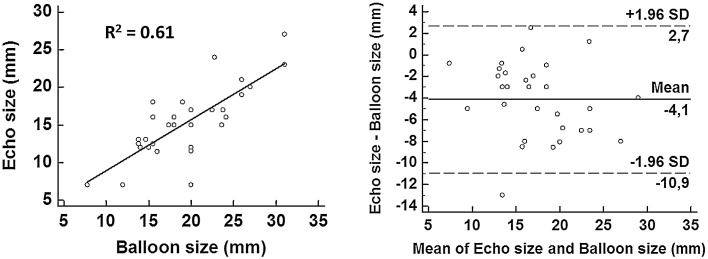
Methods: The study includes 112 procedures in 110 patients with PFO (n=75) or ASD (n=35), with use of an Amplatzer occluder, heparin and prophylactic antibiotics. Balloon sizing guided ASD-device selection. All patients received aspirin and clopidogrel for 6 months, when they all underwent TEE.
Results: All PFOs but one (98.7%) and all (100%) ASDs were successfully closed with only one complication (local pseudoaneurysm). At the 6-month TEE, there was no residual shunt in PFO patients, but 2 ASD patients had residual shunts. During long-term (4.3-year) follow-up, no stroke recurrence in PFO patients, and no other problems were encountered. Among 54 patients suffering from migraine, symptom relief or resolution was reported by 45 (83.3%) patients.
Conclusion: Percutaneous placement of an Amplatzer occluder was safe and effective with use of local anesthesia and fluoroscopy alone. There were no recurrent strokes over >4 years. Migraine relief was reported by >80% of patients.
Keywords: Amplatzer occluder; Atrial septal defect; Cryptogenic stroke; Migraine; Paradoxic embolism; Patent foramen ovale; Percutaneous closure.
Copyright © 2017. Published by Elsevier B.V.
Figures
References
-
- Butera G., Biondi-Zoccai G., Sangiorgi G. Percutaneous versus surgical closure of secundum atrial septal defects: a systematic review and meta-analysis of currently available clinical evidence. EuroIntervention. 2011;7:377–385. - PubMed
-
- Tobis J., Shenoda M. Percutaneous treatment of patent foramen ovale and atrial septal defects. J Am Coll Cardiol. 2012;60:1722–1732. - PubMed
-
- Manolis A.S. Impact of percutaneous closure of interatrial shunts on migraine attacks: single-operator series and review of the literature. Rev Recent Clin Trials. 2017;12:129–138. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
