

Actual 10-year survival after hepatic resection of colorectal liver metastases: what factors preclude cure?
- PMID: 29455841
- PMCID: PMC7439273
- DOI: 10.1016/j.surg.2018.01.004
Actual 10-year survival after hepatic resection of colorectal liver metastases: what factors preclude cure?
Abstract
Background: Hepatic resection of colorectal liver metastases is associated with long-term survival. This study analyzes actual 10-year survivors after resection of colorectal liver metastases, reports the observed rate of cure, and identifies factors that preclude cure.
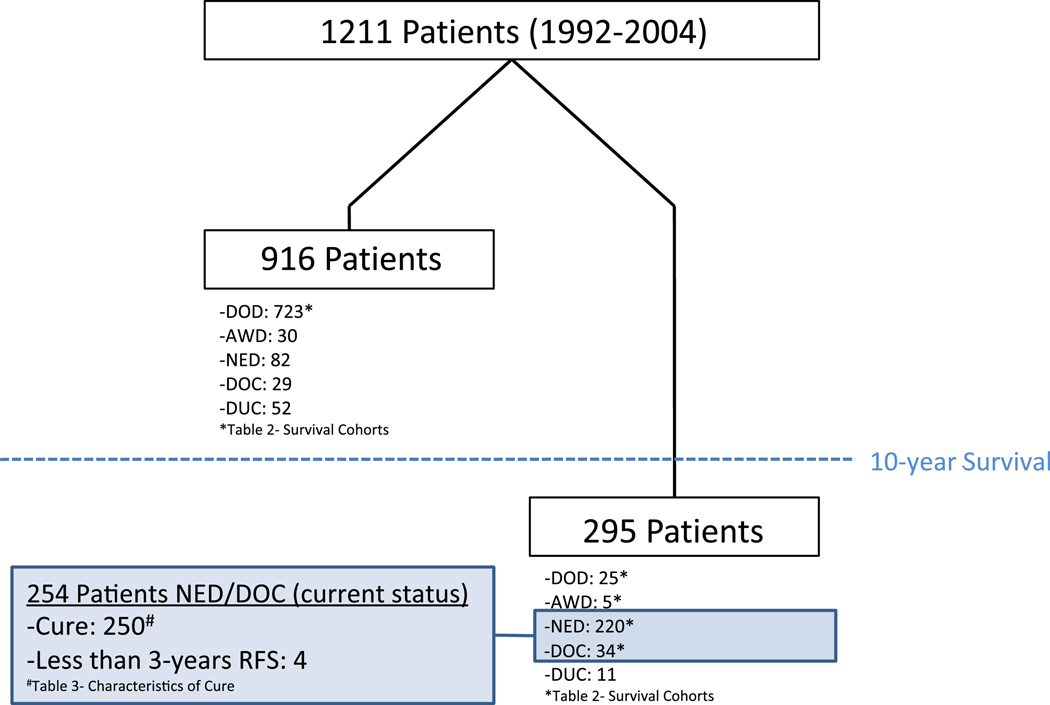
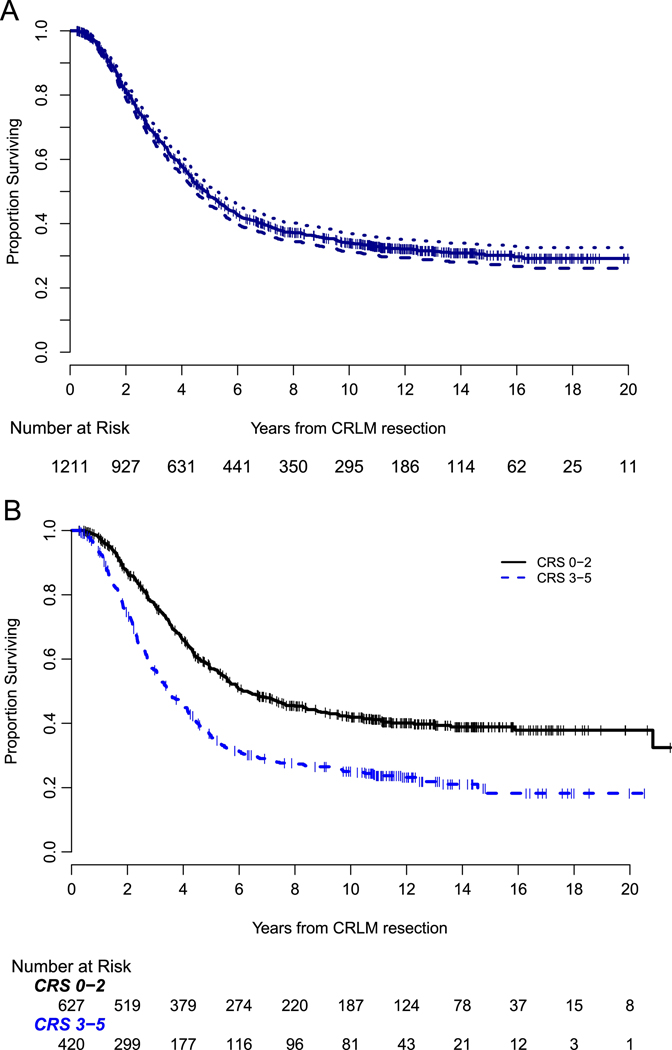
Methods: A single-institution, prospectively maintained database was queried for all initial resections for colorectal liver metastases for the years 1992-2004. Observed cure was defined as actual 10-year survival with either no recurrence or resected recurrence with at least 3 years of disease-free follow-up. Clinical risk score was dichotomized into low (0-2) and high (3-5). Semiparametric proportional hazards mixture cure model was utilized to estimate probability of cure.
Results: We included 1,211 patients with a median follow-up for survivors of 11 years. Median disease-specific survival was 4.9 years (95% CI: 4.4-5.3). 295 patients (24.4%) were actual 10-year survivors. The observed cure rate was 20.6% (n = 250). Among 250 cured patients, 192 (76.8%) had no recurrence and 58 (23.2%) had a resected recurrence with at least 3 years of disease-free follow-up. Extrahepatic disease (n = 88), carcinoembryonic antigen >200 ng/mL (n = 119), positive margin (n = 109), and >10 tumors (n = 31) had observed cure rates less than 10%. In cure model analysis, patients with both extrahepatic disease and high clinical risk score (n = 31) had an estimated probability of cure of 3.5%.
Conclusion: Actual 10-year survival after resection of colorectal liver metastases is 24% with an observed 20% cure rate. Patients with both high clinical risk score and extrahepatic disease have an estimated probability of cure less than 5%. When such factors are identified, strong consideration may be given to preoperative strategies, such as neoadjuvant chemotherapy, to help select patients for surgical therapy.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Pulitano C, Castillo F, Aldrighetti L, Bodingbauer M, Parks RW, Ferla G, et al. What defines ‘cure’ after liver resection for colorectal metastases? Results after 10 years of follow-up. HPB : the official journal of the International Hepato Pancreato Biliary Association. 2010;12:244–9. - PMC - PubMed
-
- Tomlinson JS, Jarnagin WR, DeMatteo RP, Fong Y, Kornprat P, Gonen M, et al. Actual 10-year survival after resection of colorectal liver metastases defines cure. J Clin Oncol. 2007;25:4575–80. - PubMed
-
- Vigano L, Ferrero A, Lo Tesoriere R, Capussotti L. Liver surgery for colorectal metastases: results after 10 years of follow-up. Long-term survivors, late recurrences, and prognostic role of morbidity. Annals of surgical oncology. 2008;15:2458–64. - PubMed
-
- Nordlinger B, Sorbye H, Glimelius B, Poston GJ, Schlag PM, Rougier P, et al. Perioperative FOLFOX4 chemotherapy and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC 40983): long-term results of a randomised, controlled, phase 3 trial. The Lancet Oncology. 2013;14:1208–15. - PubMed
-
- Saltz LB, Kanowitz J, Kemeny NE, Schaaf L, Spriggs D, Staton BA, et al. Phase I clinical and pharmacokinetic study of irinotecan, fluorouracil, and leucovorin in patients with advanced solid tumors. J Clin Oncol. 1996;14:2959–67. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
