

Tuberculin skin test conversion and primary progressive tuberculosis disease in the first 5 years of life: a birth cohort study from Cape Town, South Africa
- PMID: 29457055
- PMCID: PMC5810304
- DOI: 10.1016/S2352-4642(17)30149-9
Tuberculin skin test conversion and primary progressive tuberculosis disease in the first 5 years of life: a birth cohort study from Cape Town, South Africa
Abstract
Background: Tuberculosis is a leading cause of global childhood mortality. However, the epidemiology and burden of tuberculosis in infancy is not well understood. We aimed to investigate tuberculin skin test conversion and tuberculosis in the Drakenstein Child Health study, a South African birth cohort in a community in which tuberculosis incidence is hyperendemic.
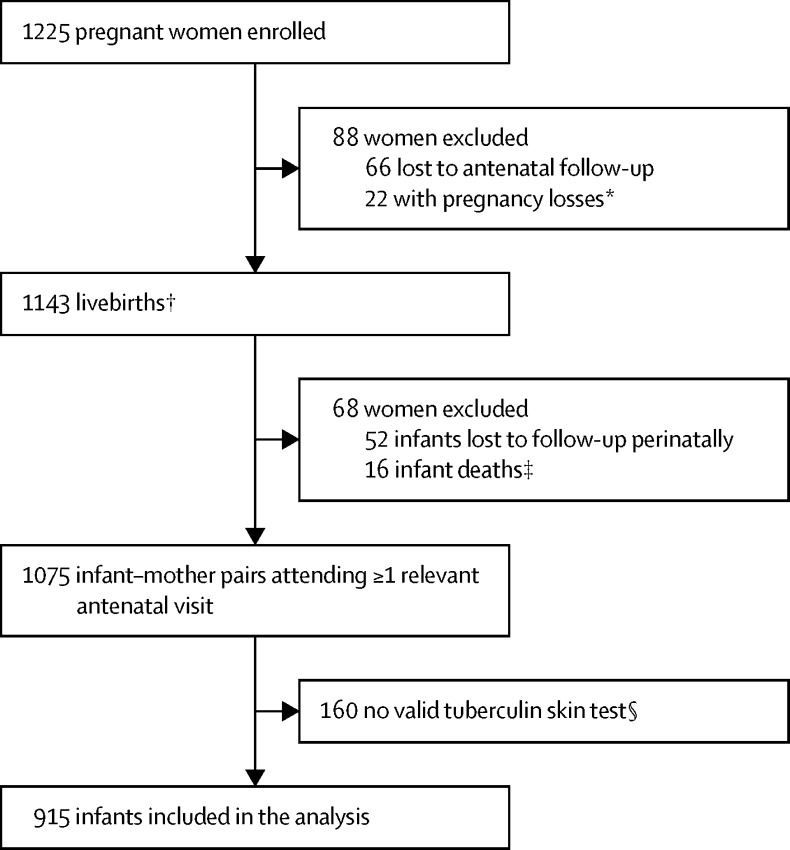
Methods: In this prospective birth cohort study, we enrolled pregnant women older than 18 years who were between 20 and 28 weeks' gestation and who were attending antenatal care in a peri-urban, impoverished South African setting. We followed up their children for tuberculosis from birth until April 1, 2017, or age 5 years. All children received BCG vaccination at birth. Tuberculin skin tests were administered to children at 6, 12, 24, 36, 48, and 60 months of age, and at the time of a lower respiratory tract infection. An induration reaction of 10 mm or more was considered to be a tuberculin skin test conversion. To prevent boosting, we censored children with a reactive, negative tuberculin skin test.
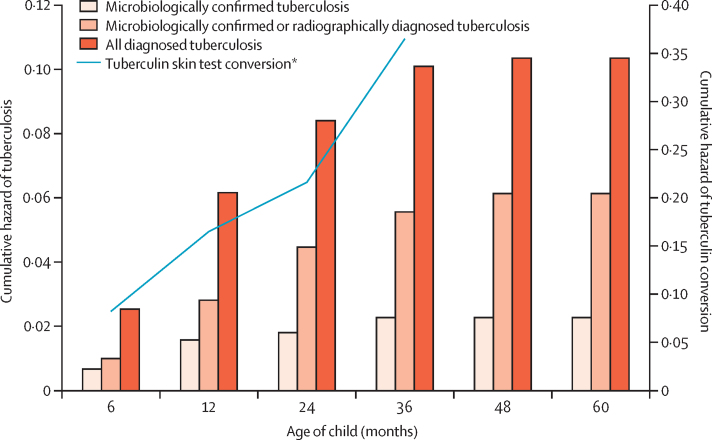
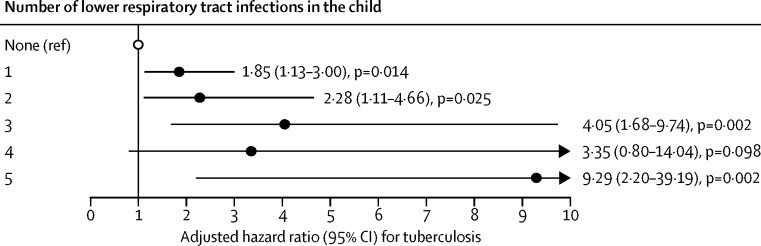
Findings: Among 915 mother-child pairs (201 [22%] HIV-positive mothers and two [<1%] HIV-positive children), 147 (16%) children had tuberculin skin test conversion, with increasing cumulative hazard with age (0·08 at 6 months, 0·17 at 12 months, 0·22 at 24 months, and 0·37 at age 36 months). For every 100 child-years, the incidence was 11·8 (95% CI 10·0-13·8) for tuberculin skin test conversion, 2·9 (2·4-3·7) for all diagnosed tuberculosis, and 0·7 (0·4-1·0) for microbiologically confirmed tuberculosis. Isoniazid preventive therapy was effective in averting disease progression (adjusted hazard ratio 0·22, 95% CI 0·08-0·63; p<0·0001). Children with a lower respiratory tract infection were significantly more likely to also have tuberculosis than were those without one (2·27, 1·42-3·62; p<0·0001).
Interpretation: Greater focus should be placed on the first years of life as a period of high burden of transmission and clinical expression of tuberculosis infection and disease. Multifaceted interventions, such as isoniazid preventive therapy and tuberculosis screening of infants with LRTIs, beginning early in life, are needed in high-burden settings.
Funding: Bill & Melinda Gates Foundation, Medical Research Council South Africa, and National Research Foundation South Africa.
Figures
Comment in
-
Mycobacterium tuberculosis infection burden in poor urban communities.Lancet Child Adolesc Health. 2018 Jan;2(1):7-8. doi: 10.1016/S2352-4642(17)30150-5. Epub 2017 Nov 20. Lancet Child Adolesc Health. 2018. PMID: 30169198 No abstract available.
References
-
- Dodd PJ, Gardiner E, Coghlan R, Seddon JA. Burden of childhood tuberculosis in 22 high-burden countries: a mathematical modelling study. Lancet Glob Health. 2014;2:e453–e459. - PubMed
-
- Drolet GJ. Present trend of case fatality rates in tuberculosis. Am Rev Tuberc Pulm Dis. 1938;37:125–151.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
