

A case of a warfarinized renal cancer patient monitored for prothrombin time-international normalized ratio during methadone introduction
- PMID: 29457079
- PMCID: PMC5804617
- DOI: 10.1186/s40981-017-0092-7
A case of a warfarinized renal cancer patient monitored for prothrombin time-international normalized ratio during methadone introduction
Abstract
Background: Warfarin, a widely used anticoagulant, interacts with various agents used in palliative care, such as oxycodone, morphine, acetaminophen, and non-steroidal anti-inflammatory drugs (NSAIDs); however, there are no reports of its interaction with methadone. We report a case of a patient receiving warfarin when methadone was introduced for pain control with monitoring of the prothrombin time-international normalized ratio (PT-INR) and deduced the pharmacological background.
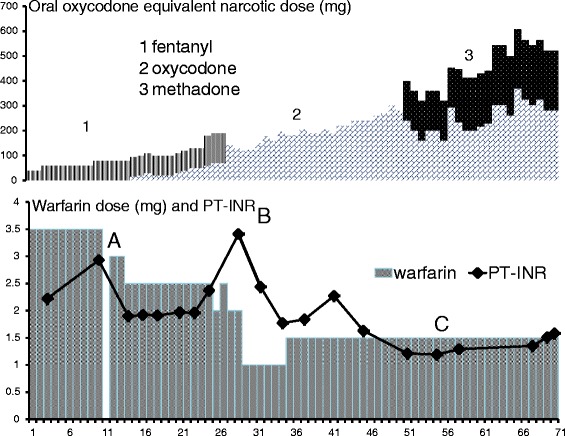
Case presentation: A 60-year-old male was emergently admitted to our university hospital for the sudden onset of severe back pain. Abdominal CT imaging revealed that the vertebral body of the ninth thoracic vertebra was occupied by bone metastasis and crushed, which caused his back pain. He received warfarin 3.5 mg/day for atrial fibrillation and tapentadol 100 mg p.o. daily for pain relief. The prothrombin time-international normalized ratio (PT-INR) was maintained at >2.2. The patient's history included diabetes mellitus and hypertension, but his laboratory test was unremarkable with the exception that his eGFR was 34 ml/min.Initially, a fentanyl dermal patch was used instead of tapentadol to avoid interactions with warfarin. We started concomitant administration of oxycodone and 2.4 g/day of acetaminophen while monitoring the PT-INR because acetaminophen increased the PT-INR to 2.93. A continuous intravenous infusion of oxycodone was introduced, in increments of the dose, resulting in an increase of the PT-INR to 3.41, which is required to reduce the dose of warfarin to 1.5 mg. Because of the lack of effective pain relief, methadone was introduced and the dose was gradually increased. The PT-INR was not changed and the dose of warfarin was not changed. An infusion of oxycodone and oral methadone was used to allow the patient to walk in his room, and he was later transferred to the palliative hospital.
Conclusions: In an oral warfarinized patient, methadone seemed to undergo different metabolism than oxycodone. When warfarin and methadone are used together, we have to consider their interaction by comparing the competitive inhibition of CYP2C9 to the induction of CYP3A4 by methadone, because CYP3A4 metabolize various drugs including oxycodone.
Keywords: CYP2B6; CYP2C9; CYP2D6; CYP3A4; Drug interaction; Methadone; Prothrombin time-international normalized ratio; Warfarin.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
[A Case with the Increased PT-INR after the Addition of Mirtazapine to Warfarin Therapy].Seishin Shinkeigaku Zasshi. 2015;117(10):820-5. Seishin Shinkeigaku Zasshi. 2015. PMID: 26827407 Japanese.
-
A Case of an Increase in Prothrombin Time-International Normalized Ratio by Interaction Between Warfarin and Baloxavir Marboxil in a Patient on Implantable Ventricular Assist Device.J Pharm Pharm Sci. 2021;24:37-40. doi: 10.18433/jpps31375. J Pharm Pharm Sci. 2021. PMID: 33460556
-
Elevated prothrombin time/international normalized ratio associated with concurrent administration of regorafenib and warfarin in a patient with advanced colorectal cancer.J Pharm Health Care Sci. 2016 Jul 8;2:15. doi: 10.1186/s40780-016-0050-y. eCollection 2016. J Pharm Health Care Sci. 2016. PMID: 27398225 Free PMC article.
-
Potential glucosamine-warfarin interaction resulting in increased international normalized ratio: case report and review of the literature and MedWatch database.Pharmacotherapy. 2008 Apr;28(4):540-8. doi: 10.1592/phco.28.4.540. Pharmacotherapy. 2008. PMID: 18363538 Review.
-
Interaction between gemfibrozil and warfarin: case report and review of the literature.Pharmacotherapy. 2009 Jun;29(6):744-8. doi: 10.1592/phco.29.6.744. Pharmacotherapy. 2009. PMID: 19476425 Review.
References
-
- Overholser BR, Foster DR. Opioid pharmacokinetic drug–drug interactions. Am J Manag Care. 2011;17(11):276–287. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous