

Effects of glucose-insulin infusion during major oral and maxillofacial surgery on postoperative complications and outcomes
- PMID: 29457119
- PMCID: PMC5804688
- DOI: 10.1186/s40981-018-0148-3
Effects of glucose-insulin infusion during major oral and maxillofacial surgery on postoperative complications and outcomes
Abstract
Background: Secretion of hormones, which antagonize the action of insulin, is facilitated in response to surgery, and acute resistance to the action of insulin develops. Our aim is to elucidate the effects of intraoperative glycemic control by glucose-insulin (GI) infusion on postoperative complications and outcomes in major oral and maxillofacial surgery.
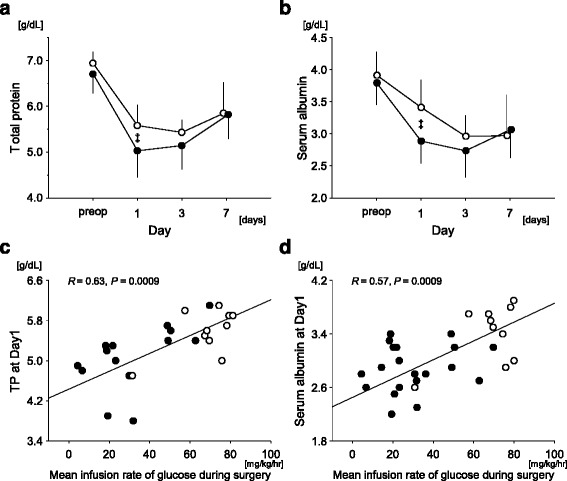
Findings: Thirty patients aged ≥ 60 years undergoing a radical operation of oral malignant tumors with tissue reconstruction (≥ 8 h) were analyzed. In the GI group, regular insulin was continuously applied with glucose-added acetate Ringer's solution (5-10 g glucose per 500 mL). Blood glucose was adjusted within the target concentration of 80-120 mg/dL. In the control group, combination of acetate Ringer's solution containing 1% (W/V) glucose and lactate Ringer's solution, which contains no glucose, was employed. Perioperative clinical parameters, incidence of hypoalbuminemia, and postoperative complications, i.e., surgical site infection, necrosis of a reconstructed flap, bacteremia, hypotension, or pneumonia, were compared. Both serum total protein and albumin concentrations (postoperative day 1 [Day1]) were higher in the GI group. The mean infusion rate of glucose during surgery (mg/kg/h) was independently associated with the decrease in both serum total protein and albumin concentrations from the control to Day1. No difference was found between the groups in the incidence of postoperative complications and the days required until discharge, except less incidence of hypoalbuminemia in the GI group.
Conclusions: Application of additional glucose during major oral and maxillofacial surgery preserved serum albumin concentration. However, it did not lead to less postoperative complications and less days until discharge.
Keywords: Hypoalbuminemia; Inflammation; Postoperative complication; Surgical diabetes.
Conflict of interest statement
This study was conducted with approval from the Ethics Committee of Kagoshima University Medical and Dental Hospital (no. 297). This study was registered in the University Hospital Medical Information Network Clinical Trials Registry (UMIN-CTR), UMIN000015522. Written informed consent was obtained from all patients prior to participation.The authors declare that they have no competing interests.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources