

Critical Care Pharmacists and Medication Management in an ICU Recovery Center
- PMID: 29457491
- PMCID: PMC6039256
- DOI: 10.1177/1060028018759343
Critical Care Pharmacists and Medication Management in an ICU Recovery Center
Abstract
Background: Many patients experience complications following critical illness; these are now widely referred to as post-intensive care syndrome (PICS). An interprofessional intensive care unit (ICU) recovery center (ICU-RC), also known as a PICS clinic, is one potential approach to promoting patient and family recovery following critical illness.
Objectives: To describe the role of an ICU-RC critical care pharmacist in identifying and treating medication-related problems among ICU survivors.
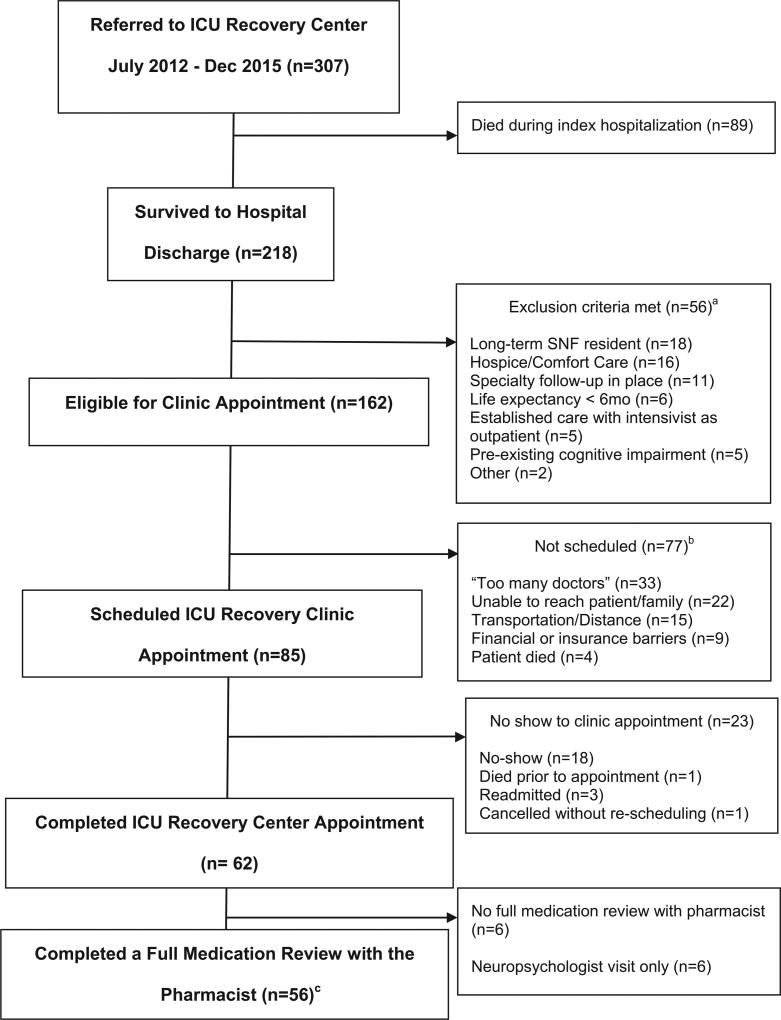
Methods: A prospective, observational cohort study was conducted of all outpatient appointments of a tertiary care hospital's ICU-RC between July 2012 and December 2015. The pharmacist completed a full medication review, including medication reconciliation, interview, counseling, and resultant interventions, during the ICU-RC appointment.
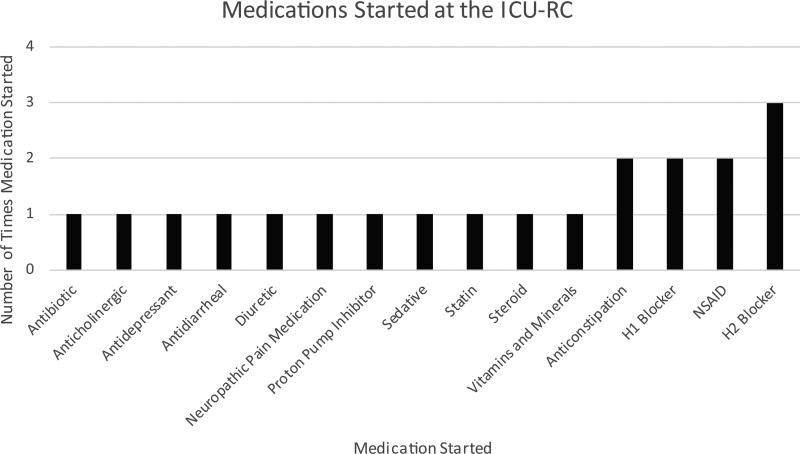
Results: Data from all completed ICU-RC visits were analyzed (n = 62). A full medication review was performed in 56 (90%) of these patients by the pharmacist. The median number of pharmacy interventions per patient was 4 (interquartile range = 2, 5). All 56 patients had at least 1 pharmacy intervention; 22 (39%) patients had medication(s) stopped at the clinic appointment, and 18 (32%) patients had new medication(s) started. The pharmacist identified 9 (16%) patients who had an adverse drug event (ADE); 18 (32%) patients had ADE preventive measures instituted. An influenza vaccination was administered to 13 (23%) patients despite an inpatient protocol to ensure influenza vaccination prior to discharge. A pneumococcal vaccination was administered to 2 (4%) patients.
Conclusions: Use of a critical care pharmacist resulted in the identification and treatment of multiple medication-related problems in an ICU-RC as well as implementation of preventive measures.
Keywords: adverse drug event; medication reconciliation; pharmacist; post–intensive care syndrome; post–intensive care syndrome clinic.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Joanna L. Stollings, Sarah L. Bloom, Li Wang, and James Jackson have no conflicts of interest to disclose; E. Wesley Ely has received honoraria for CME activities from Pfizer, Abbott, and Orion and grant support from Dr Franz Kohler Chemie GmbH; Carla M. Sevin has no conflicts of interest to disclose.
Figures

Comment in
-
Reply: Critical Care Pharmacists and Medication Management in an ICU Recovery Center.Ann Pharmacother. 2019 Jan;53(1):106. doi: 10.1177/1060028018799501. Epub 2018 Sep 1. Ann Pharmacother. 2019. PMID: 30175590 No abstract available.
-
Comment: Critical Care Pharmacists and Medication Management in an ICU Recovery Center.Ann Pharmacother. 2019 Jan;53(1):105. doi: 10.1177/1060028018799290. Epub 2018 Sep 6. Ann Pharmacother. 2019. PMID: 30187762 No abstract available.
References
-
- Needham DM, Davidson J, Cohen H, et al. Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders’ conference. Crit Care Med. 2012;40:502–509. - PubMed
-
- Jackson JC, Hart RP, Gordon SM, et al. Six-month neuropsychological outcome of medical intensive care unit patients. Crit Care Med. 2003;31:1226–1234. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
