

Training nurses in a competency framework to support adults with epilepsy and intellectual disability: the EpAID cluster RCT
- PMID: 29457585
- PMCID: PMC6485678
- DOI: 10.3310/hta22100
Training nurses in a competency framework to support adults with epilepsy and intellectual disability: the EpAID cluster RCT
Abstract
Background: People with an intellectual (learning) disability (ID) and epilepsy have an increased seizure frequency, higher frequencies of multiple antiepileptic drug (AED) use and side effects, higher treatment costs, higher mortality rates and more behavioural problems than the rest of the population with epilepsy. The introduction of nurse-led care may lead to improvements in outcome for those with an ID and epilepsy; however, this has not been tested in a definitive clinical trial.
Objective: To determine whether or not ID nurses, using a competency framework developed to optimise nurse management of epilepsy in people with an ID, can cost-effectively improve clinical and quality-of-life outcomes in the management of epilepsy compared with treatment as usual.
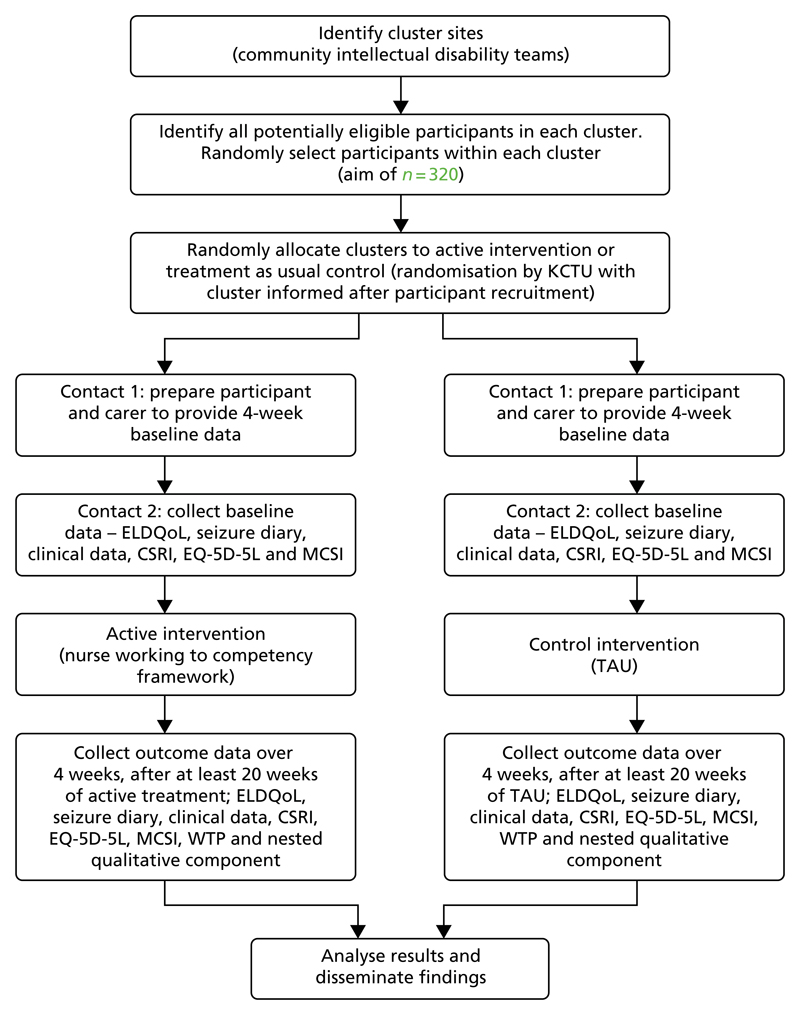
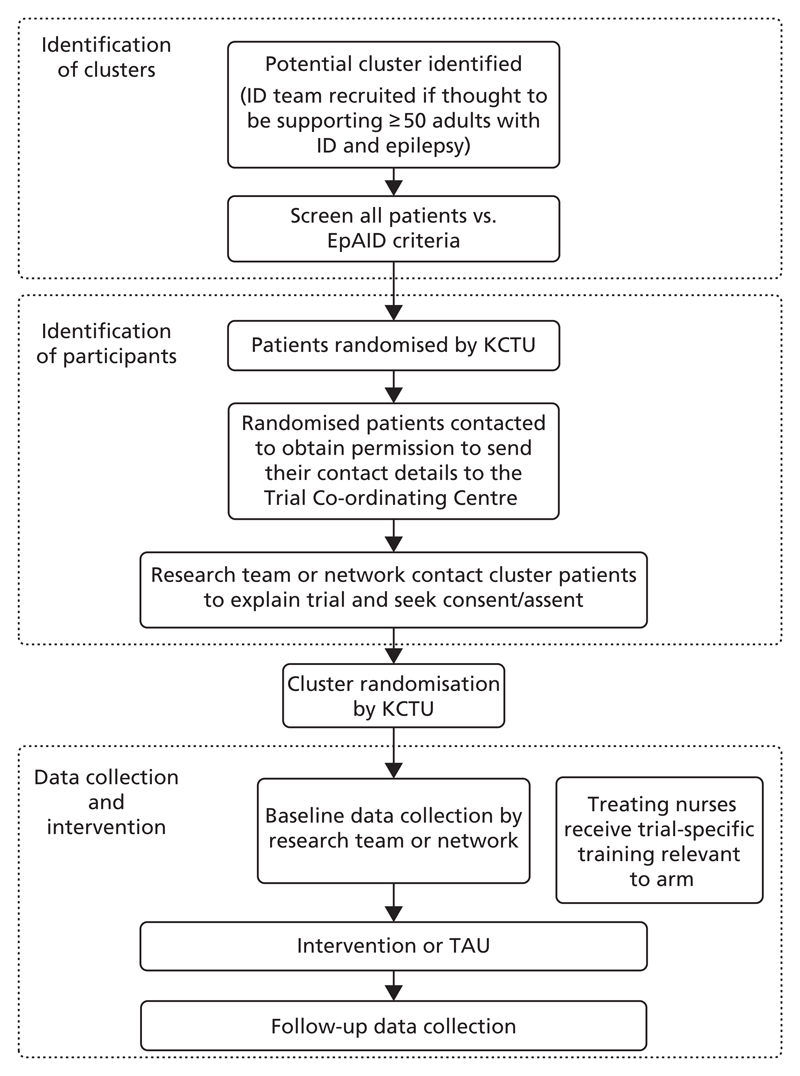
Design: Cluster-randomised two-arm trial.
Setting: Community-based secondary care delivered by members of community ID teams.
Participants: Participants were adults aged 18-65 years with an ID and epilepsy under the care of a community ID team and had had at least one seizure in the 6 months before the trial.
Interventions: The experimental intervention was the Learning Disability Epilepsy Specialist Nurse Competency Framework. This provides guidelines describing a structure and goals to support the delivery of epilepsy care and management by ID-trained nurses.
Main outcome measures: The primary outcome was the seizure severity scale from the Epilepsy and Learning Disabilities Quality of Life questionnaire. Measures of mood, behaviour, AED side effects and carer strain were also collected. A cost-utility analysis was undertaken along with a qualitative examination of carers' views of participants' epilepsy management.
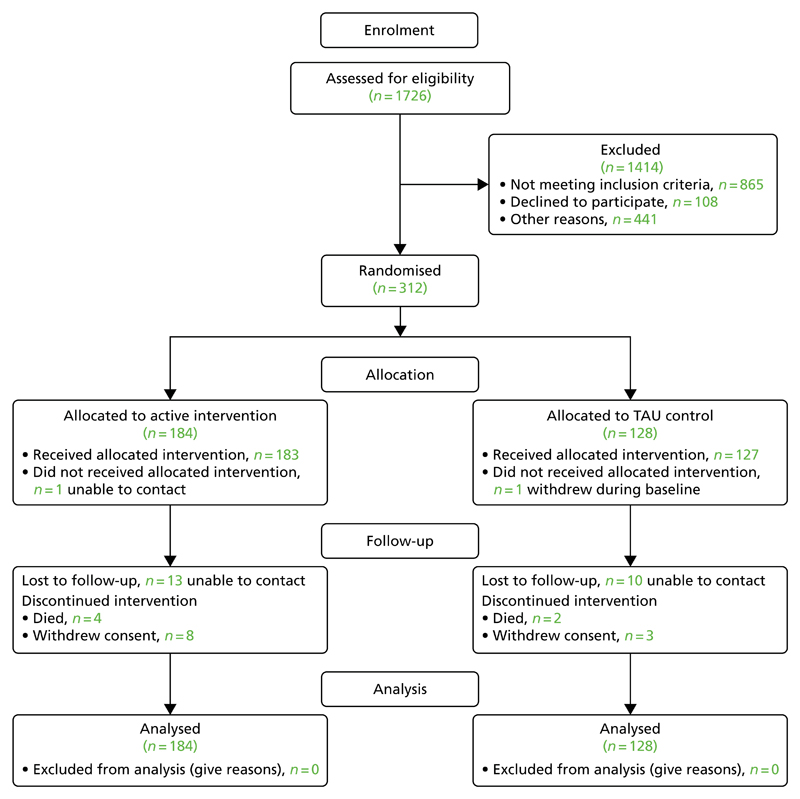
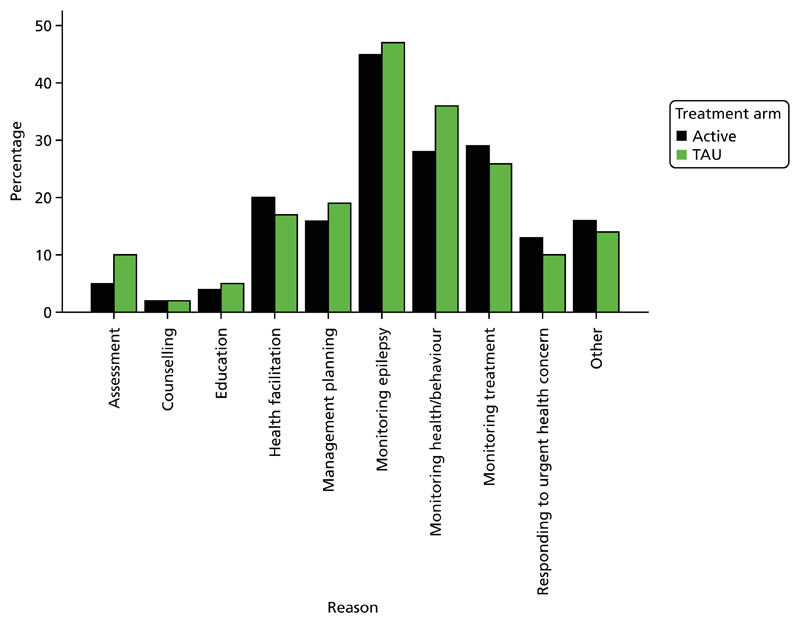
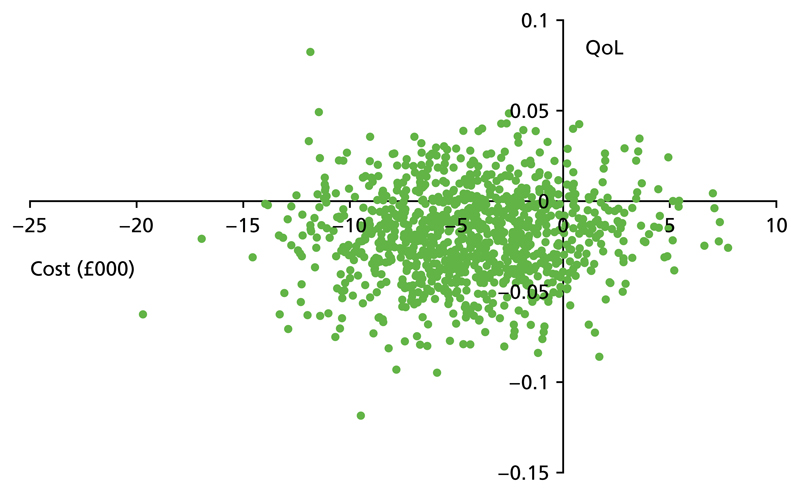
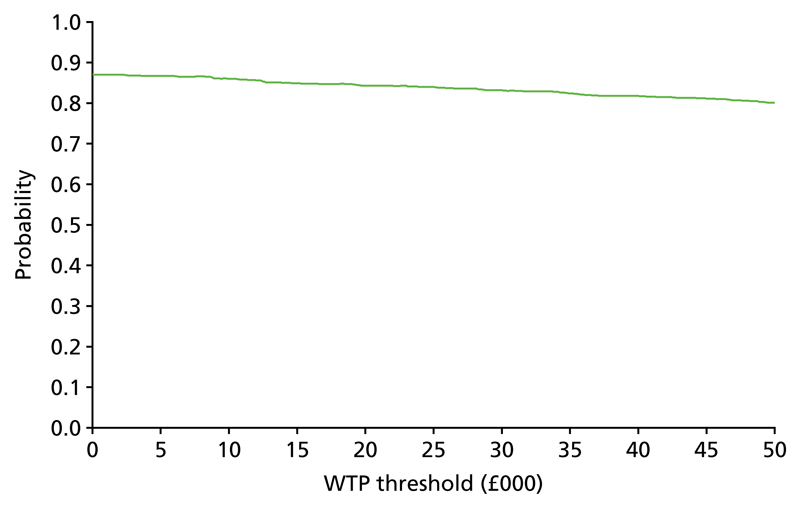
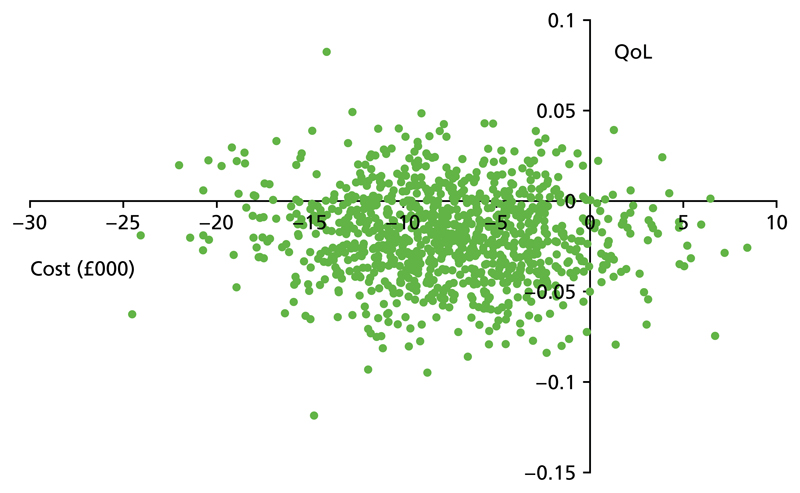
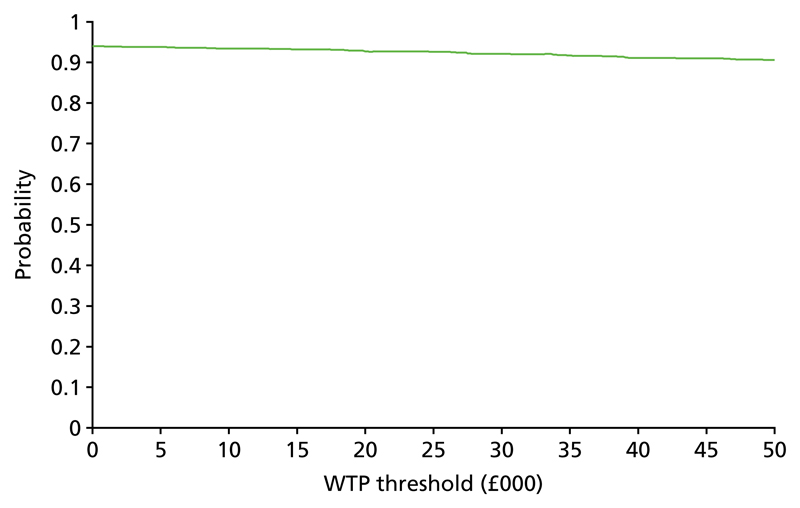
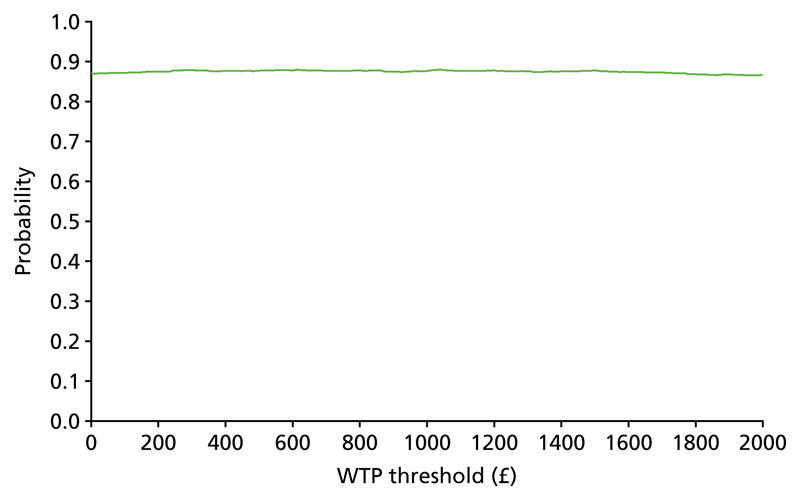
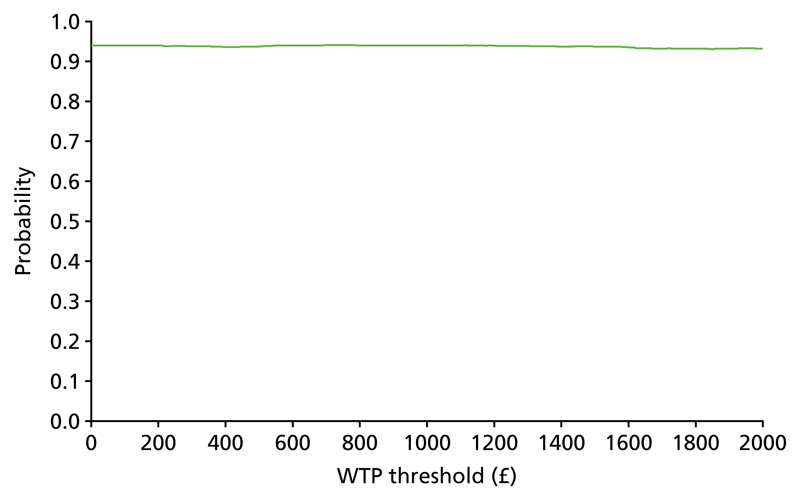
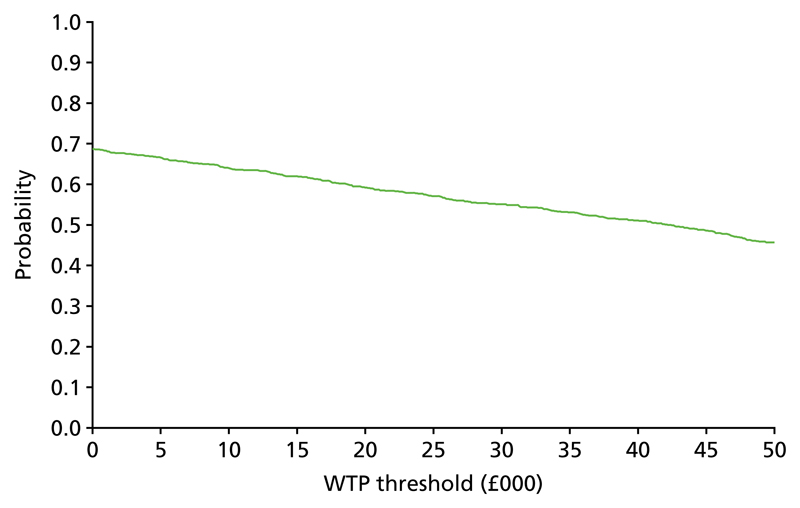
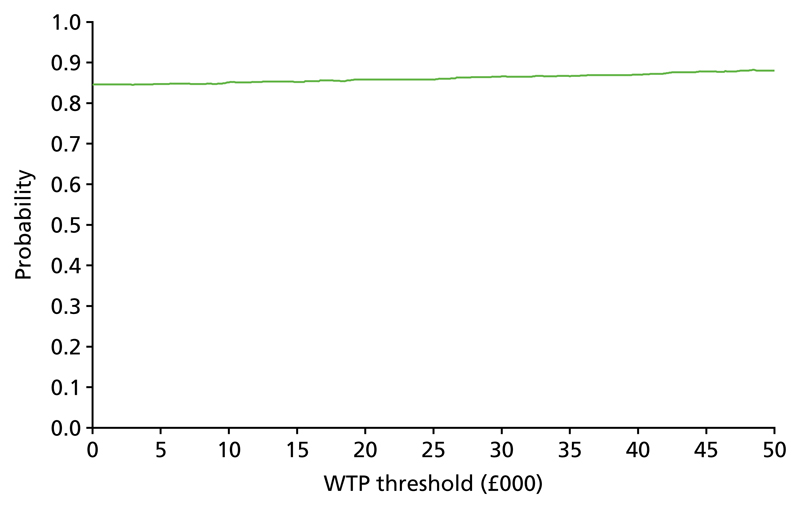
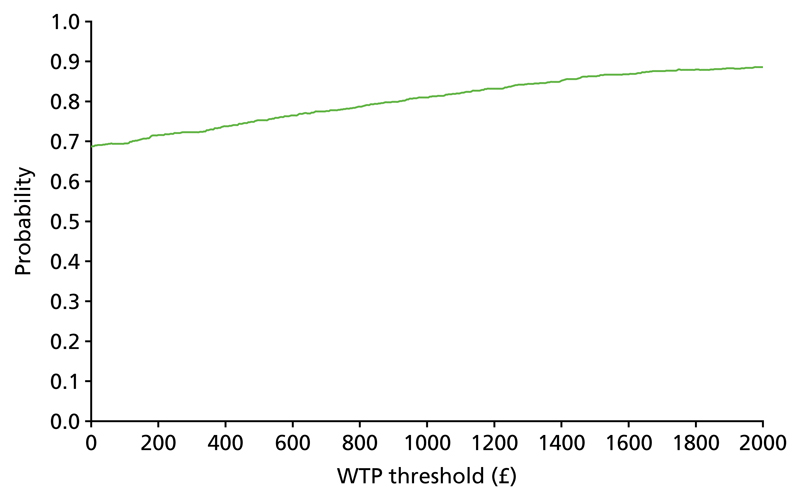
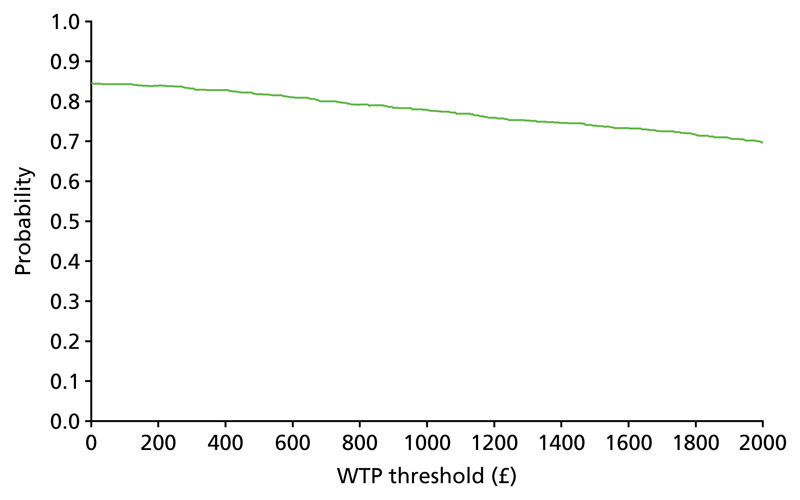
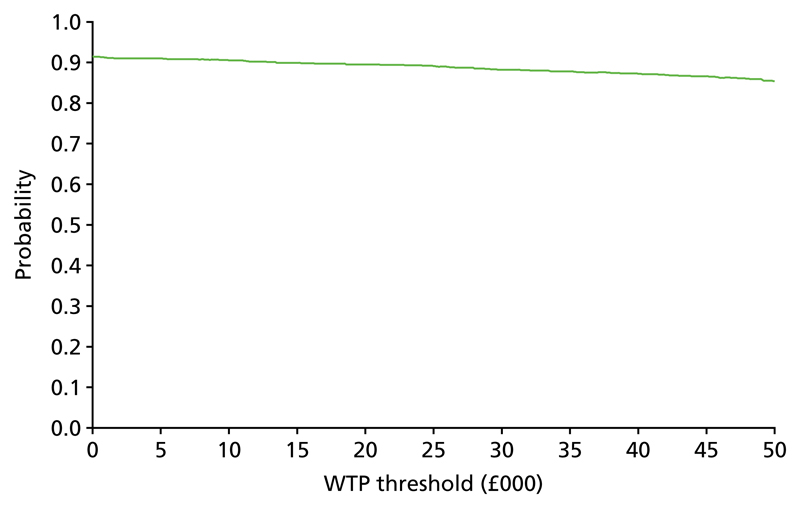
Results: In total, 312 individuals were recruited into the study from 17 research clusters. Using an intention-to-treat analysis controlling for baseline individual-level and cluster-level variables there was no significant difference in seizure severity score between the two arms. Altogether, 238 complete cases were included in the non-imputed primary analysis. Analyses of the secondary outcomes revealed no significant differences between arms. A planned subgroup analysis identified a significant interaction between treatment arm and level of ID. There was a suggestion in those with mild to moderate ID that the competency framework may be associated with a small reduction in concerns over seizure severity (standard error 2.005, 95% confidence interval -0.554 to 7.307; p = 0.092). However, neither subgroup showed a significant intervention effect individually. Family members' perceptions of nurses' management depended on the professional status of the nurses, regardless of trial arm. Economic analysis suggested that the competency framework intervention was likely to be cost-effective, primarily because of a reduction in the costs of supporting participants compared with treatment as usual.
Limitations: The intervention could not be delivered blinded. Treatment as usual varied widely between the research sites.
Conclusions: Overall, for adults with an ID and epilepsy, the framework conferred no clinical benefit compared with usual treatment. The economic analysis suggested that there may be a role for the framework in enhancing the cost-effectiveness of support for people with epilepsy and an ID. Future research could explore the specific value of the competency framework for those with a mild to moderate ID and the potential for greater long-term benefits arising from the continuing professional development element of the framework.
Trial registration: Current Controlled Trials ISRCTN96895428.
Funding: This trial was funded by the NIHR Health Technology Assessment programme and will be published in full in Health Technology Assessment; Vol. 22, No. 10. See the NIHR Journals Library website for further project information.
Conflict of interest statement
During the preparation of this report Howard Ring was the chairperson of the Health Technology Assessment Mental, Psychological and Occupational Health Panel and he was a member of the Psychological and Community Therapies Panel during the project. Cam Donaldson was a member of the Medical Research Council Methodology Research Panel.
Figures
References
-
- Ring H, Gilbert N, Hook R, Platt A, Smith C, Irvine F, et al. Improving outcomes in adults with epilepsy and intellectual disability (EpAID) using a nurse-led intervention: study protocol for a cluster randomised controlled trial. Trials. 2016;17:297. doi: 10.1186/s13063-016-1429-7. - DOI - PMC - PubMed
-
- Kerr M. Epilepsy and Learning Disability. In: Rugg-Gunn FJ, Sander JW, Smalls JE, editors. Epilepsy 2011: From Science to Society. Chalfont: International League Against Epilepsy and Epilepsy Society; 2011. pp. 407–417.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
