

Impact of Arterial Stiffness on WatchPAT Variables in Patients With Obstructive Sleep Apnea
- PMID: 29458701
- PMCID: PMC5837833
- DOI: 10.5664/jcsm.6970
Impact of Arterial Stiffness on WatchPAT Variables in Patients With Obstructive Sleep Apnea
Abstract
Study objectives: The WatchPAT is a wrist-worn portable device that creates integration data regarding peripheral arterial tone (PAT), oxyhemoglobin saturation, heart rate, and actigraphy to diagnose or screen for obstructive sleep apnea (OSA). Previous studies have demonstrated the efficacy and validity of respiratory variables measured by the WatchPAT compared to those using polysomnography (PSG). However, the effects of arterial stiffness or atherosclerosis on WatchPAT parameters remain to be elucidated.
Methods: Sixty-one consecutive patients with suspected OSA who underwent home-based testing with the WatchPAT 200, standard in-laboratory overnight polysomnography (PSG), and pulse wave velocity (PWV) as an index of arterial stiffness were studied. All PSG recordings were scored manually using the American Academy of Sleep Medicine criteria, whereas WatchPAT data were analyzed by an automatic algorithm. We evaluated how arterial stiffness affected respiratory event index data in WatchPAT (WP-AHI), because WP-AHI could be partly influenced by PAT, comparing WP-AHI and the apneahypopnea index measured by PSG (PSG-AHI) in consideration of PWV result.
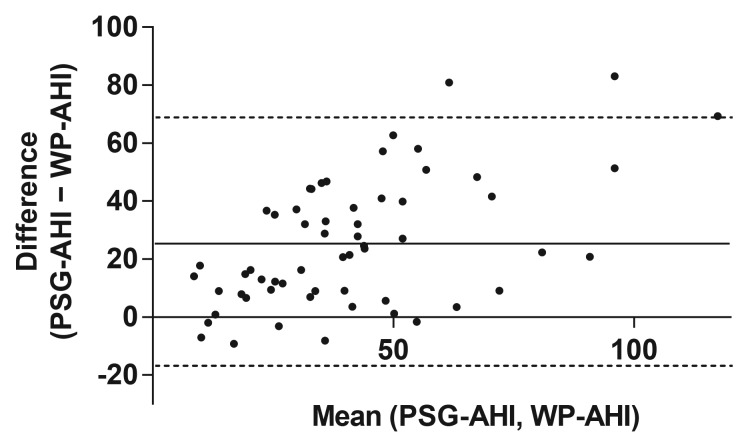
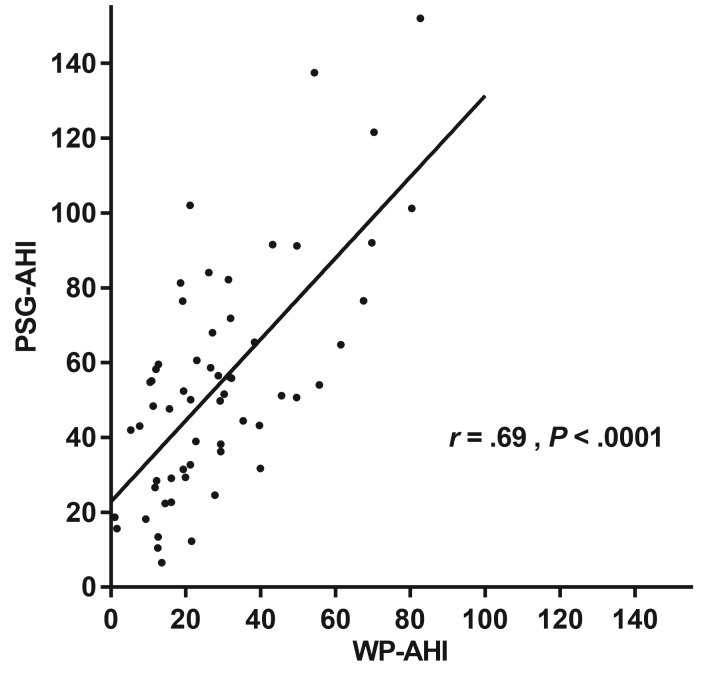
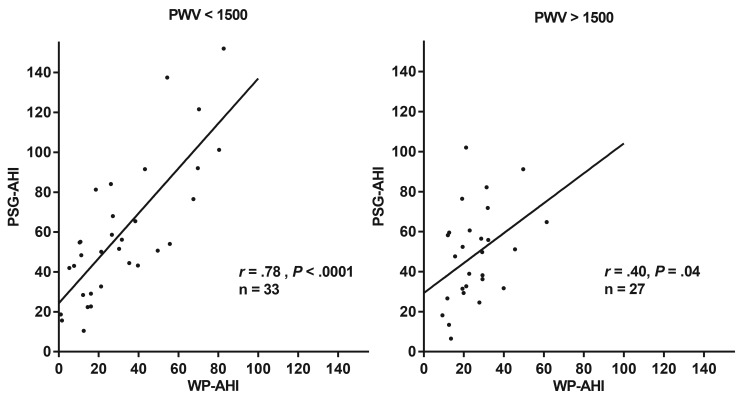
Results: Overall, WP-AHI was moderately correlated to PSG-AHI, but WP-AHI was significantly lower than PSG-AHI (28.4 ± 19.2 versus 53.6 ± 30.2 events/h, P < .0001). For the lower PWV group, there was a significant correlation and good agreement between the WP-AHI and PSG-AHI, but as the PWV increased, there was low correlation between the WP-AHI and PSG-AHI.
Conclusions: Arterial stiffness may affect the respiratory variables measured by WatchPAT in patients with OSA.
Commentary: A commentary on this article appears in this issue on page 301.
Keywords: WatchPAT; apnea-hypopnea index; arterial stiffness; obstructive sleep apnea; pulse wave velocity.
© 2018 American Academy of Sleep Medicine.
Figures
References
-
- Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353(19):2034–2041. - PubMed
-
- Choi JH, Kim EJ, Kim YS, et al. Validation study of portable device for the diagnosis of obstructive sleep apnea according to the new AASM scoring criteria: Watch-PAT 100. Acta Otolaryngol. 2010;130(7):838–843. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
