

Psychiatric Symptom Dimensions Are Associated With Dissociable Shifts in Metacognition but Not Task Performance
- PMID: 29458997
- PMCID: PMC6117452
- DOI: 10.1016/j.biopsych.2017.12.017
Psychiatric Symptom Dimensions Are Associated With Dissociable Shifts in Metacognition but Not Task Performance
Abstract
Background: Distortions in metacognition-the ability to reflect on and control other cognitive processes-are thought to be characteristic of poor mental health. However, it remains unknown whether such shifts in self-evaluation are due to specific alterations in metacognition and/or a downstream consequence of changes in decision-making processes.
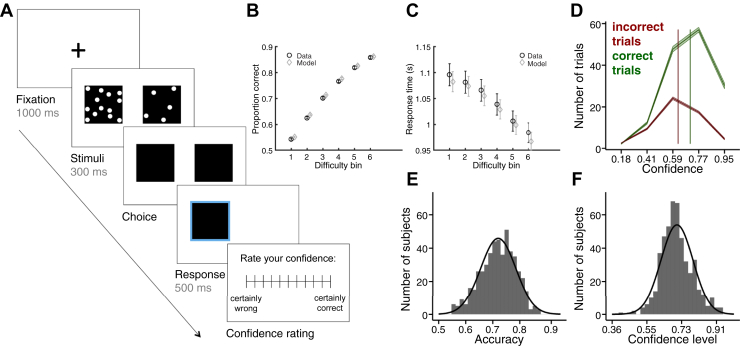
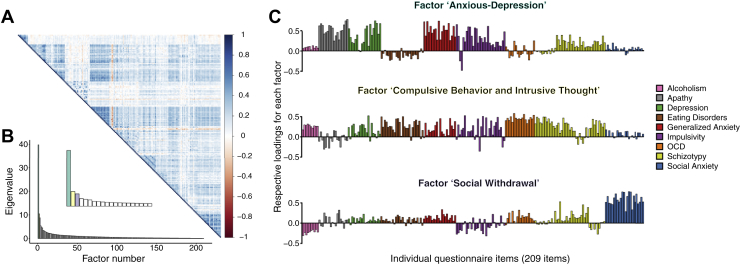
Methods: Using perceptual decision making as a model system, we employed a computational psychiatry approach to relate parameters governing both decision formation and metacognitive evaluation to self-reported transdiagnostic symptom dimensions in a large general population sample (N = 995).
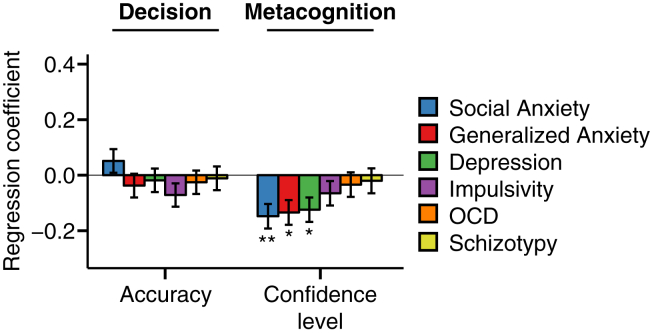
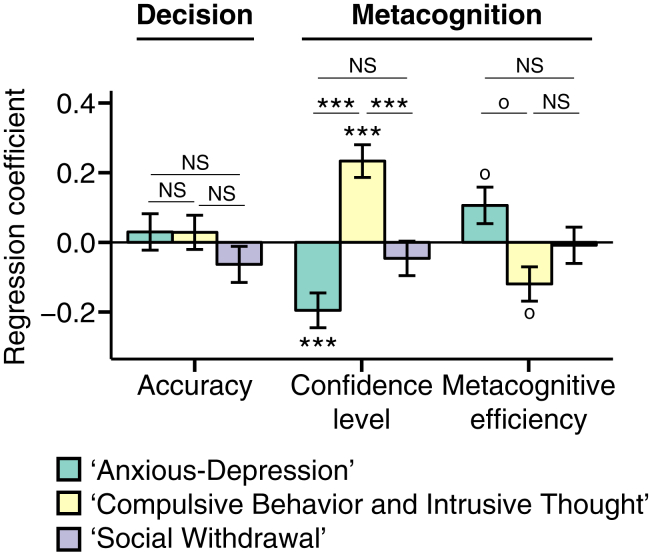
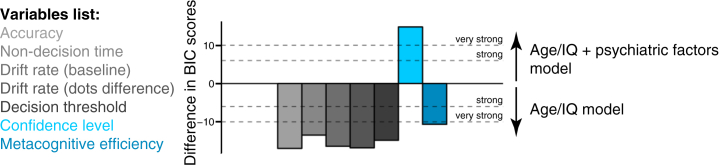
Results: Variability in psychopathology was unrelated to either speed or accuracy of decision formation. In contrast, leveraging a dimensional approach, we revealed independent relationships between psychopathology and metacognition: a symptom dimension related to anxiety and depression was associated with lower confidence and heightened metacognitive efficiency, whereas a dimension characterizing compulsive behavior and intrusive thoughts was associated with higher confidence and lower metacognitive efficiency. Furthermore, we obtained a robust double dissociation-whereas psychiatric symptoms predicted changes in metacognition but not decision performance, age predicted changes in decision performance but not metacognition.
Conclusions: Our findings indicate a specific and pervasive link between metacognition and mental health. Our study bridges a gap between an emerging neuroscience of decision making and an understanding of metacognitive alterations in psychopathology.
Keywords: Cognitive neuroscience; Computational psychiatry; Confidence; Decision making; Metacognition; Psychopathology.
Copyright © 2018 Society of Biological Psychiatry. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Confidence biases in problem gambling.J Behav Addict. 2024 Jun 7;13(2):650-664. doi: 10.1556/2006.2024.00030. Print 2024 Jun 26. J Behav Addict. 2024. PMID: 38850516 Free PMC article.
-
Explaining distortions in metacognition with an attractor network model of decision uncertainty.PLoS Comput Biol. 2021 Jul 26;17(7):e1009201. doi: 10.1371/journal.pcbi.1009201. eCollection 2021 Jul. PLoS Comput Biol. 2021. PMID: 34310613 Free PMC article.
-
Sure I'm Sure: Prefrontal Oscillations Support Metacognitive Monitoring of Decision Making.J Neurosci. 2017 Jan 25;37(4):781-789. doi: 10.1523/JNEUROSCI.1612-16.2016. J Neurosci. 2017. PMID: 28123015 Free PMC article.
-
Dysfunctional metacognition across psychopathologies: A meta-analytic review.Eur Psychiatry. 2017 Sep;45:139-153. doi: 10.1016/j.eurpsy.2017.05.029. Epub 2017 Jun 7. Eur Psychiatry. 2017. PMID: 28763680 Review.
-
[Characteristics and impact of metacognitive deficits in schizophrenia].Encephale. 2013 Apr;39(2):123-9. doi: 10.1016/j.encep.2012.01.009. Epub 2012 Dec 6. Encephale. 2013. PMID: 23219408 Review. French.
Cited by
-
I know that I know. But do I know that I do not know?Front Psychol. 2023 Feb 23;14:1128200. doi: 10.3389/fpsyg.2023.1128200. eCollection 2023. Front Psychol. 2023. PMID: 36910778 Free PMC article.
-
Advice-taking as a bridge between decision neuroscience and mental capacity.Int J Law Psychiatry. 2019 Nov-Dec;67:101504. doi: 10.1016/j.ijlp.2019.101504. Epub 2019 Nov 26. Int J Law Psychiatry. 2019. PMID: 31785723 Free PMC article. Review.
-
Preserved metacognition despite impaired perception of intentionality cues in schizophrenia.Schizophr Res Cogn. 2021 Sep 9;27:100215. doi: 10.1016/j.scog.2021.100215. eCollection 2022 Mar. Schizophr Res Cogn. 2021. PMID: 34692428 Free PMC article.
-
Differences in metacognitive functioning between obsessive-compulsive disorder patients and highly compulsive individuals from the general population.Psychol Med. 2023 Dec;53(16):7933-7942. doi: 10.1017/S003329172300209X. Epub 2023 Aug 9. Psychol Med. 2023. PMID: 37553980 Free PMC article.
-
Metacognition as a window into subjective affective experience.Psychiatry Clin Neurosci. 2024 Aug;78(8):430-437. doi: 10.1111/pcn.13683. Epub 2024 Jun 17. Psychiatry Clin Neurosci. 2024. PMID: 38884177 Free PMC article. Review.
References
-
- Wells A., Fisher P., Myers S., Wheatley J., Patel T., Brewin C.R. Metacognitive therapy in treatment-resistant depression: A platform trial. Behav Res Ther. 2012;50:367–373. - PubMed
-
- Bandura A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol Rev. 1977;84:191. - PubMed
-
- Elliott R., Sahakian B.J., McKay A.P., Herrod J.J., Robbins T.W., Paykel E.S. Neuropsychological impairments in unipolar depression: The influence of perceived failure on subsequent performance. Psychol Med. 1996;26:975–989. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
