

Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms
- PMID: 29459239
- PMCID: PMC5953551
- DOI: 10.1016/j.cjca.2017.12.005
Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms
Abstract
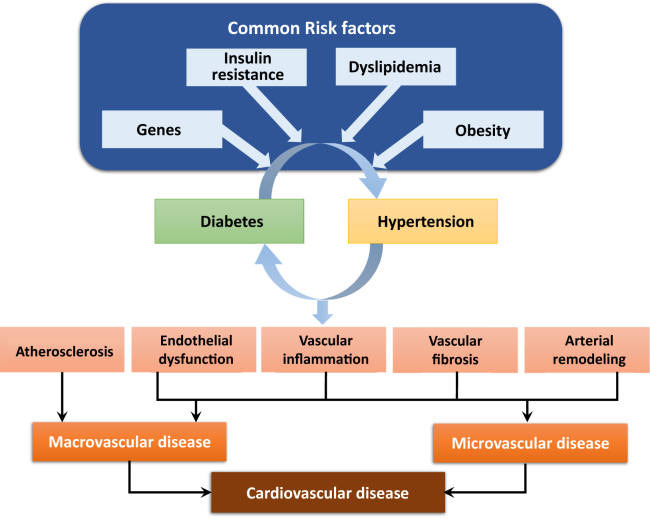
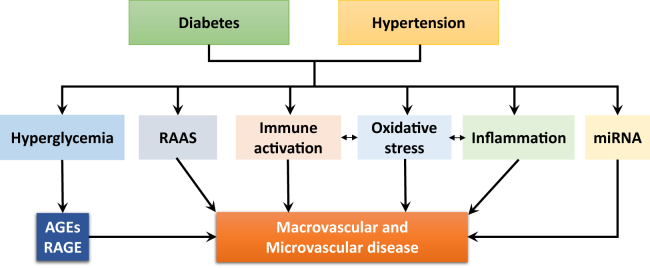
Hypertension and type 2 diabetes are common comorbidities. Hypertension is twice as frequent in patients with diabetes compared with those who do not have diabetes. Moreover, patients with hypertension often exhibit insulin resistance and are at greater risk of diabetes developing than are normotensive individuals. The major cause of morbidity and mortality in diabetes is cardiovascular disease, which is exacerbated by hypertension. Accordingly, diabetes and hypertension are closely interlinked because of similar risk factors, such as endothelial dysfunction, vascular inflammation, arterial remodelling, atherosclerosis, dyslipidemia, and obesity. There is also substantial overlap in the cardiovascular complications of diabetes and hypertension related primarily to microvascular and macrovascular disease. Common mechanisms, such as upregulation of the renin-angiotensin-aldosterone system, oxidative stress, inflammation, and activation of the immune system likely contribute to the close relationship between diabetes and hypertension. In this article we discuss diabetes and hypertension as comorbidities and discuss the pathophysiological features of vascular complications associated with these conditions. We also highlight some vascular mechanisms that predispose to both conditions, focusing on advanced glycation end products, oxidative stress, inflammation, the immune system, and microRNAs. Finally, we provide some insights into current therapies targeting diabetes and cardiovascular complications and introduce some new agents that may have vasoprotective therapeutic potential in diabetes.
L’hypertension et le diabète de type 2 sont des affections concomitantes fréquentes. L’hypertension est deux fois plus fréquente chez les patients atteints de diabète que chez ceux qui n’en sont pas atteints. De plus, les patients atteints d’hypertension sont souvent résistants à l’insuline et sont plus susceptibles de souffrir de diabète que les personnes normotendues. Chez les diabétiques, la principale cause de morbidité et de mortalité est la maladie cardiovasculaire, qui est exacerbée par l’hypertension. En conséquence, le diabète et l’hypertension sont étroitement interreliés en raison de facteurs de risques similaires, comme la dysfonction endothéliale, l’inflammation vasculaire, le remodelage artériel, l’athérosclérose, la dyslipidémie et l’obésité. On observe un chevauchement important entre les complications cardiovasculaires du diabète et celles de l’hypertension liées principalement à des maladies microvasculaires et macrovasculaires. Des mécanismes communs, comme une stimulation du système rénine-angiotensine-aldostérone, un stress oxydatif, une inflammation et une activation du système immunitaire, sont susceptibles de contribuer à la relation étroite entre le diabète et l’hypertension. Dans cet article, nous abordons le diabète et l’hypertension comme des affections concomitantes et nous parlons des caractéristiques physiopathologiques des complications vasculaires associées à ces affections. Nous soulignons également certains mécanismes vasculaires qui prédisposent à ces deux affections, en mettant l’accent sur les produits finaux de glycation avancée, le stress oxydatif, l’inflammation, le système immunitaire et les micro-ARN. Finalement, nous présentons certaines connaissances sur les traitements actuels ciblant le diabète et les complications cardiovasculaires et nous présentons de nouveaux agents qui pourraient avoir un pouvoir vasoprotecteur chez les patients diabétiques.
Copyright © 2017 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ogurtsova K., da Rocha Fernandes J.D., Huang Y. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. 2017;128:40–50. - PubMed
-
- Mitchell B.D., Stern M.P., Haffner S.M., Hazuda H.P., Patterson J.K. Risk factors for cardiovascular mortality in Mexican Americans and non-Hispanic whites. San Antonio Heart Study. Am J Epidemiol. 1990;131:423–433. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
