

Los Angeles Motor Scale to Identify Large Vessel Occlusion: Prehospital Validation and Comparison With Other Screens
- PMID: 29459391
- PMCID: PMC5829024
- DOI: 10.1161/STROKEAHA.117.019228
Los Angeles Motor Scale to Identify Large Vessel Occlusion: Prehospital Validation and Comparison With Other Screens
Abstract
Background and purpose: Prehospital scales have been developed to identify patients with acute cerebral ischemia (ACI) because of large vessel occlusion (LVO) for direct routing to Comprehensive Stroke Centers (CSCs), but few have been validated in the prehospital setting, and their impact on routing of patients with intracranial hemorrhage has not been delineated. The purpose of this study was to validate the Los Angeles Motor Scale (LAMS) for LVO and CSC-appropriate (LVO ACI and intracranial hemorrhage patients) recognition and compare the LAMS to other scales.
Methods: The performance of the LAMS, administered prehospital by paramedics to consecutive ambulance trial patients, was assessed in identifying (1) LVOs among all patients with ACI and (2) CSC-appropriate patients among all suspected strokes. Additionally, the LAMS administered postarrival was compared concurrently with 6 other scales proposed for paramedic use and the full National Institutes of Health Stroke Scale.
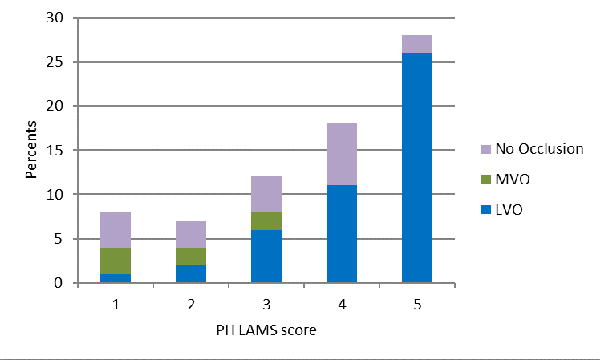
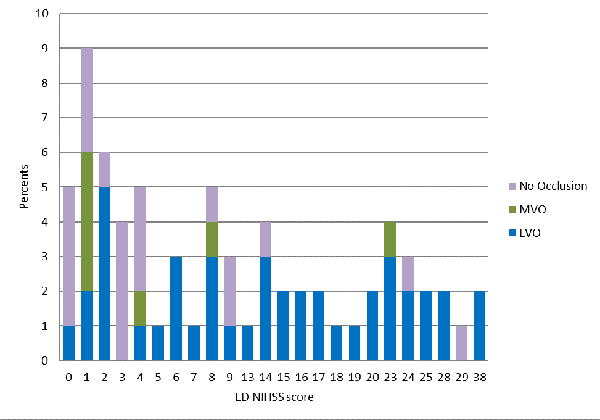
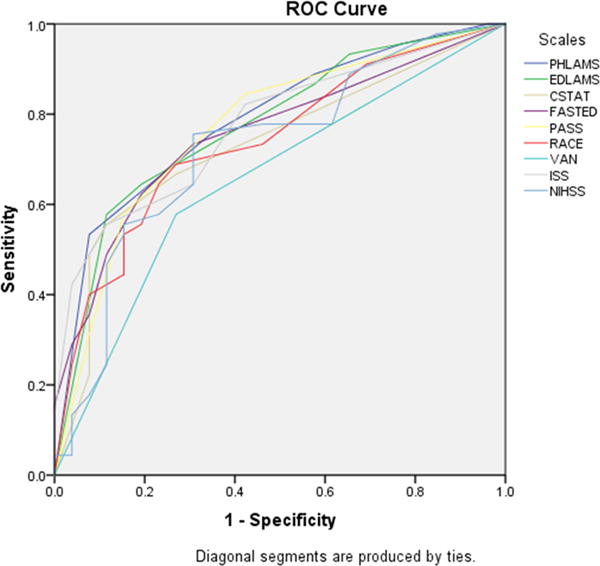
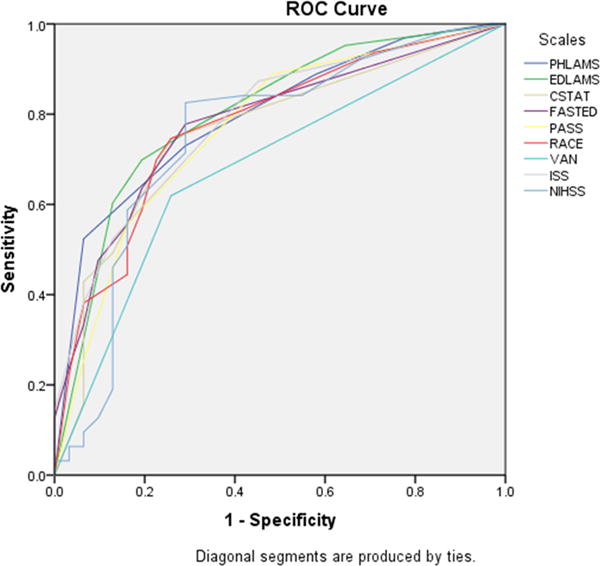
Results: Among 94 patients, age was 70 (±13) and 49% female. Final diagnoses were ACI in 76% (because of LVO in 48% and non-LVO in 28%), intracranial hemorrhage in 19%, and neurovascular mimic in 5%. The LAMS administered by paramedics in the field performed moderately well in identifying LVO among patients with ACI (C statistic, 0.79; accuracy, 0.72) and CSC-appropriate among all suspected stroke transports (C statistic, 0.80; accuracy, 0.72). When concurrently performed in the emergency department postarrival, the LAMS showed comparable or better accuracy versus the 7 comparator scales, for LVO among ACI (accuracies LAMS, 0.70; other scales, 0.62-0.68) and CSC-appropriate (accuracies LAMS, 0.73; other scales, 0.56-0.73).
Conclusions: The LAMS performed in the field by paramedics identifies LVO and CSC-appropriate patients with good accuracy. The LAMS performs comparably or better than more extended prehospital scales and the full National Institutes of Health Stroke Scale.
Keywords: ambulances; brain ischemia; cerebral hemorrhage; thrombectomy; triage.
© 2018 American Heart Association, Inc.
Conflict of interest statement
Figures
References
-
- Alberts MJ, Latchaw RE, Selman WR, Shephard T, Hadley MN, Brass LM, et al. Recommendations for comprehensive stroke centers: A consensus statement from the brain attack coalition. Stroke. 2005;36:1597–1616. - PubMed
-
- Higashida R, Alberts MJ, Alexander DN, Crocco TJ, Demaerschalk BM, Derdeyn CP, et al. Interactions within stroke systems of care: A policy statement from the american heart association/american stroke association. Stroke. 2013;44:2961–2984. - PubMed
-
- Saver JL, Goyal M, van der Lugt A, Menon BK, Majoie CB, Dippel DW, et al. Time to treatment with endovascular thrombectomy and outcomes from ischemic stroke: A meta-analysis. JAMA. 2016;316:1279–1288. - PubMed
-
- American Heart/Stroke Association Mission Lifeline Stroke Committee. Severity-based stroke triage algorithm for ems. 2017:2017.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
