

Predictors of Thrombolysis Administration in Mild Stroke: Florida-Puerto Rico Collaboration to Reduce Stroke Disparities
- PMID: 29459397
- PMCID: PMC5829011
- DOI: 10.1161/STROKEAHA.117.019341
Predictors of Thrombolysis Administration in Mild Stroke: Florida-Puerto Rico Collaboration to Reduce Stroke Disparities
Abstract
Background and purpose: Mild stroke is the most common cause for thrombolysis exclusion in patients acutely presenting to the hospital. Thrombolysis administration in this subgroup is highly variable among different clinicians and institutions. We aim to study the predictors of thrombolysis in patients with mild ischemic stroke in the FL-PR CReSD registry (Florida-Puerto Rico Collaboration to Reduce Stroke Disparities).
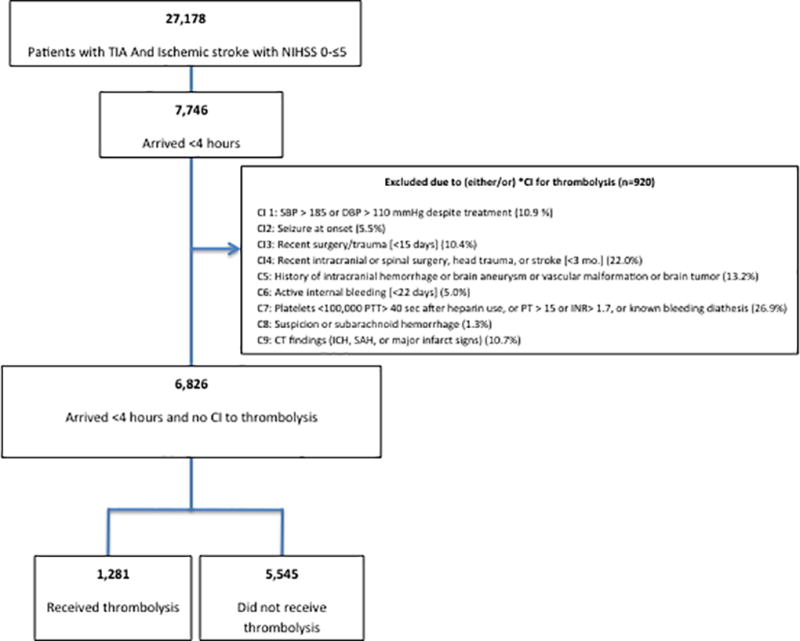
Methods: Among 73 712 prospectively enrolled patients with a final diagnosis of ischemic stroke or TIA from January 2010 to April 2015, we identified 7746 cases with persistent neurological symptoms and National Institutes of Health Stroke Scale ≤5 who arrived within 4 hours of symptom onset. Multilevel logistic regression analysis with generalized estimating equations was used to identify independent predictors of thrombolytic administration in the subgroup of patients without contraindications to thrombolysis.
Results: We included 6826 cases (final diagnosis mild stroke, 74.6% and TIA, 25.4%). Median age was 72 (interquartile range, 21); 52.7% men, 70.3% white, 12.9% black, 16.8% Hispanic; and median National Institutes of Health Stroke Scale, 2 (interquartile range, 3). Patients who received thrombolysis (n=1281, 18.7%) were younger (68 versus 72 years), had less vascular risk factors (hypertension, diabetes mellitus, and dyslipidemia), had lower risk of prior vascular disease (myocardial infarction, peripheral vascular disease, and previous stroke), and had a higher presenting median National Institutes of Health Stroke Scale (4 versus 2). In the multilevel multivariable model, early hospital arrival (arrive by 0-2 hours versus ≥3.5 hours; odds ratio [OR], 8.16; 95% confidence interval [CI], 4.76-13.98), higher National Institutes of Health Stroke Scale (OR, 1.87; 95% CI, 1.77-1.98), aphasia at presentation (OR, 1.35; 95% CI, 1.12-1.62), faster door-to-computed tomography time (OR, 1.81; 95% CI, 1.53-2.15), and presenting to an academic hospital (OR, 2.02; 95% CI, 1.39-2.95) were independent predictors of thrombolysis administration.
Conclusions: Mild acutely presenting stroke patients are more likely to receive thrombolysis if they are young, white, or Hispanic and arrive early to the hospital with more severe neurological presentation. Identification of predictors of thrombolysis is important in design of future studies to assess the use of thrombolysis for mild stroke.
Keywords: Florida; Puerto Rico; risk factors; stroke; therapy.
© 2018 American Heart Association, Inc.
Figures
References
-
- Smith EE, Fonarow GC, Reeves MJ, Cox M, Olson DM, Hernandez AF, et al. Outcomes in mild or rapidly improving stroke not treated with intravenous recombinant tissue-type plasminogen activator: Findings from get with the guidelines-stroke. Stroke; a journal of cerebral circulation. 2011;42:3110–3115. - PubMed
-
- Nedeltchev K, Schwegler B, Haefeli T, Brekenfeld C, Gralla J, Fischer U, et al. Outcome of stroke with mild or rapidly improving symptoms. Stroke; a journal of cerebral circulation. 2007;38:2531–2535. - PubMed
-
- Smith EE, Abdullah AR, Petkovska I, Rosenthal E, Koroshetz WJ, Schwamm LH. Poor outcomes in patients who do not receive intravenous tissue plasminogen activator because of mild or improving ischemic stroke. Stroke; a journal of cerebral circulation. 2005;36:2497–2499. - PubMed
-
- Romano JG, Smith EE, Liang L, Gardener H, Campo-Bustillo I, Khatri P, et al. Distinct short-term outcomes in patients with mild versus rapidly improving stroke not treated with thrombolytics. Stroke; a journal of cerebral circulation. 2016;47:1278–1285. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
