

Sex Difference in Patients With Ischemic Heart Failure Undergoing Surgical Revascularization: Results From the STICH Trial (Surgical Treatment for Ischemic Heart Failure)
- PMID: 29459462
- PMCID: PMC5896331
- DOI: 10.1161/CIRCULATIONAHA.117.030526
Sex Difference in Patients With Ischemic Heart Failure Undergoing Surgical Revascularization: Results From the STICH Trial (Surgical Treatment for Ischemic Heart Failure)
Abstract
Background: Female sex is conventionally considered a risk factor for coronary artery bypass grafting (CABG) and has been included as a poor prognostic factor in multiple cardiac operative risk evaluation scores. We aimed to investigate the association of sex and the long-term benefit of CABG in patients with ischemic left ventricular dysfunction enrolled in the prospective STICH trial (Surgical Treatment for Ischemic Heart Failure Study).
Methods: The STICH trial randomized 1212 patients (148 [12%] women and 1064 [88%] men) with coronary artery disease and left ventricular ejection fraction ≤35% to CABG+medical therapy (MED) versus MED alone. Long-term (10-year) outcomes with each treatment were compared according to sex.
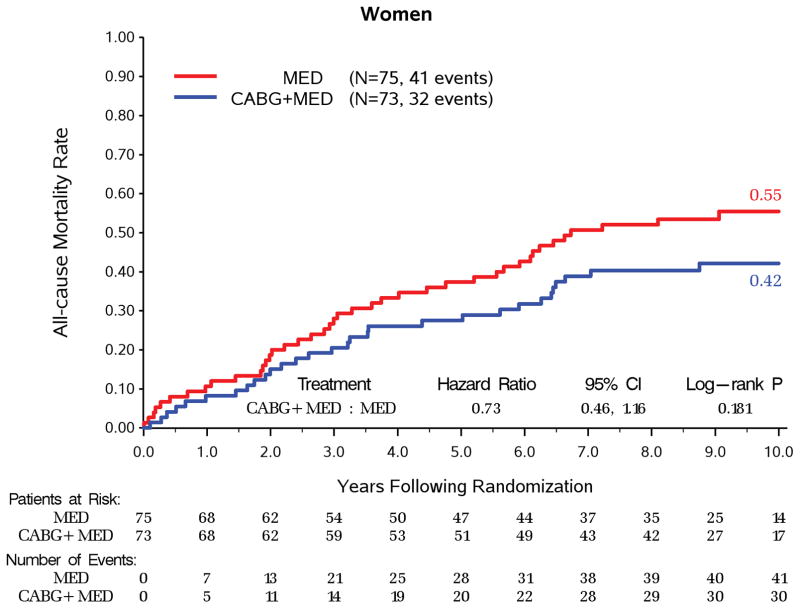
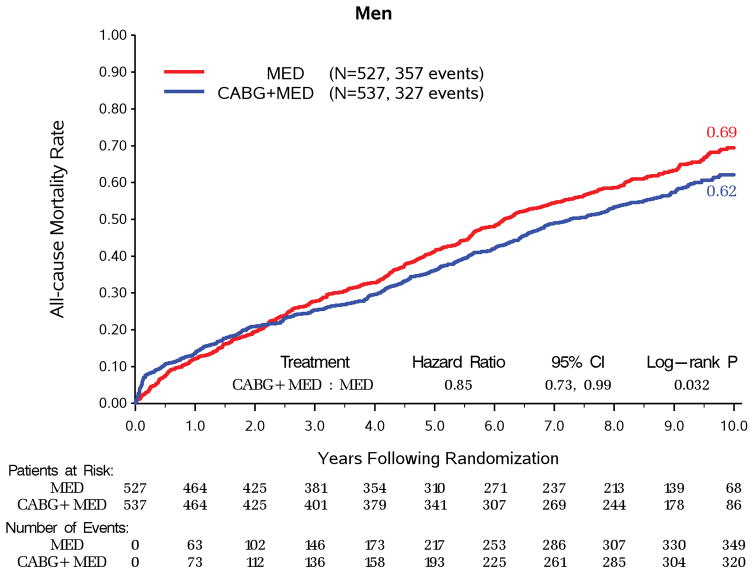
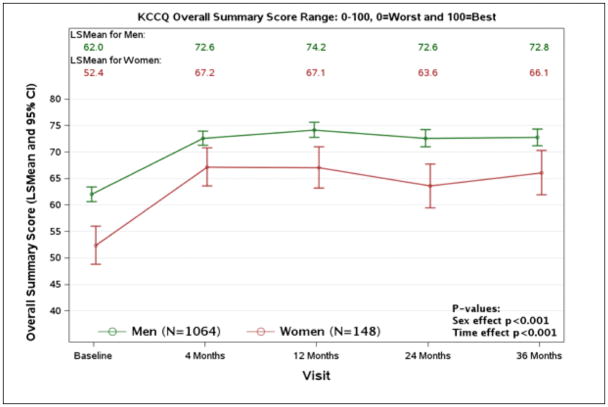
Results: At baseline, women were older (63.4 versus 59.3 years; P=0.016) with higher body mass index (27.9 versus 26.7 kg/m2; P=0.001). Women had more coronary artery disease risk factors (diabetes mellitus, 55.4% versus 37.2%; hypertension, 70.9% versus 58.6%; hyperlipidemia, 70.3% versus 58.9%) except for smoking (13.5% versus 21.8%) and had lower rates of prior CABG (0% versus 3.4%; all P<0.05) than men. Moreover, women had higher New York Heart Association class (class III/IV, 66.2% versus 57.0%), lower 6-minute walk capacity (300 versus 350 m), and lower Kansas City Cardiomyopathy Questionnaire overall summary scores (51 versus 63; all P<0.05). Over 10 years of follow-up, all-cause mortality (49.0% versus 65.8%; adjusted hazard ratio, 0.67; 95% confidence interval, 0.52-0.86; P=0.002) and cardiovascular mortality (34.3% versus 52.3%; adjusted hazard ratio, 0.65; 95% confidence interval, 0.48-0.89; P=0.006) were significantly lower in women compared with men. With randomization to CABG+MED versus MED treatment, there was no significant interaction between sex and treatment group in all-cause mortality, cardiovascular mortality, or the composite of all-cause mortality or cardiovascular hospitalization (all P>0.05). In addition, surgical deaths were not statistically different (1.5% versus 5.1%; P=0.187) between sexes among patients randomized to CABG per protocol as initial treatment.
Conclusions: Sex is not associated with the effect of CABG+MED versus MED on all-cause mortality, cardiovascular mortality, the composite of death or cardiovascular hospitalization, or surgical deaths in patients with ischemic left ventricular dysfunction. Thus, sex should not influence treatment decisions about CABG in these patients.
Clinical trial registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT00023595.
Keywords: coronary artery bypass; heart failure; women.
© 2018 American Heart Association, Inc.
Figures
Comment in
-
Sauce for the Goose Versus Sauce for the Gander: Should Men and Women Play the Same Game But With Different Rules?Circulation. 2018 Feb 20;137(8):791-793. doi: 10.1161/CIRCULATIONAHA.118.033168. Circulation. 2018. PMID: 29459464 No abstract available.
-
Sex and mortality associated with coronary artery bypass graft.J Thorac Dis. 2018 Jul;10(Suppl 18):S2157-S2159. doi: 10.21037/jtd.2018.06.149. J Thorac Dis. 2018. PMID: 30123548 Free PMC article. No abstract available.
-
Female gender and left ventricular dysfunction in myocardial surgical revascularization: the strange couple.J Thorac Dis. 2018 Jul;10(Suppl 18):S2160-S2164. doi: 10.21037/jtd.2018.06.42. J Thorac Dis. 2018. PMID: 30123549 Free PMC article. No abstract available.
-
Gender and surgical revascularization: there is a light at the end of the tunnel?J Thorac Dis. 2018 Jul;10(Suppl 18):S2202-S2205. doi: 10.21037/jtd.2018.06.145. J Thorac Dis. 2018. PMID: 30123561 Free PMC article. No abstract available.
-
Both sexes should be treated equally: sex difference in patients with ischemic heart failure undergoing surgical revascularization.J Thorac Dis. 2018 Sep;10(Suppl 26):S3153-S3154. doi: 10.21037/jtd.2018.08.26. J Thorac Dis. 2018. PMID: 30370102 Free PMC article. No abstract available.
References
-
- O’Meara E, Clayton T, McEntegart MB, McMurray JJ, Pina IL, Granger CB, Ostergren J, Michelson EL, Solomon SD, Pocock S, Yusuf S, Swedberg K, Pfeffer MA Investigators C. Sex differences in clinical characteristics and prognosis in a broad spectrum of patients with heart failure: results of the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) program. Circulation. 2007;115:3111–20. - PubMed
-
- Ghali JK, Krause-Steinrauf HJ, Adams KF, Khan SS, Rosenberg YD, Yancy CW, Young JB, Goldman S, Peberdy MA, Lindenfeld J. Gender differences in advanced heart failure: insights from the BEST study. J Am Coll Cardiol. 2003;42:2128–34. - PubMed
-
- Ghali JK, Pina IL, Gottlieb SS, Deedwania PC, Wikstrand JC, Group M-HS. Metoprolol CR/XL in female patients with heart failure: analysis of the experience in Metoprolol Extended-Release Randomized Intervention Trial in Heart Failure (MERIT-HF) Circulation. 2002;105:1585–91. - PubMed
-
- Hsich EM, Pina IL. Heart failure in women: a need for prospective data. J Am Coll Cardiol. 2009;54:491–8. - PubMed
-
- Shaw LJ, Bairey Merz CN, Pepine CJ, Reis SE, Bittner V, Kelsey SF, Olson M, Johnson BD, Mankad S, Sharaf BL, Rogers WJ, Wessel TR, Arant CB, Pohost GM, Lerman A, Quyyumi AA, Sopko G Investigators W. Insights from the NHLBI-Sponsored Women’s Ischemia Syndrome Evaluation (WISE) Study: Part I: gender differences in traditional and novel risk factors, symptom evaluation, and gender-optimized diagnostic strategies. J Am Coll Cardiol. 2006;47:S4–S20. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
