

Evidence Underpinning the Centers for Medicare & Medicaid Services' Severe Sepsis and Septic Shock Management Bundle (SEP-1): A Systematic Review
- PMID: 29459977
- PMCID: PMC11146290
- DOI: 10.7326/M17-2947
Evidence Underpinning the Centers for Medicare & Medicaid Services' Severe Sepsis and Septic Shock Management Bundle (SEP-1): A Systematic Review
Erratum in
-
Correction: Severe Sepsis and Septic Shock Management Bundle.Ann Intern Med. 2018 Apr 17;168(8):612. doi: 10.7326/L18-0132. Ann Intern Med. 2018. PMID: 29677263 No abstract available.
Abstract
This article has been corrected. To see what has changed, please read the Letter to the Editor and the authors' response. The original version (PDF) is appended to this article as a Supplement.
Background: The Severe Sepsis and Septic Shock Early Management Bundle (SEP-1), the sepsis performance measure introduced in 2015 by the Centers for Medicare & Medicaid Services (CMS), requires the reporting of up to 5 hemodynamic interventions, as many as 141 tasks, and 3 hours to document for a single patient.
Purpose: To evaluate whether moderate- or high-level evidence shows that use of the 2015 SEP-1 or its hemodynamic interventions improves survival in adults with sepsis.
Data sources: PubMed, Embase, Scopus, Web of Science, and ClinicalTrials.gov from inception to 28 November 2017 with no language restrictions.
Study selection: Randomized and observational studies of death among adults with sepsis who received versus those who did not receive either the entire SEP-1 bundle or 1 or more SEP-1 hemodynamic interventions, including serial lactate measurements; a fluid infusion of 30 mL/kg of body weight; and assessment of volume status and tissue perfusion with a focused examination, bedside cardiovascular ultrasonography, or fluid responsiveness testing.
Data extraction: Two investigators independently extracted study data and assessed each study's risk of bias; 4 authors rated level of evidence by consensus using CMS criteria published in 2013. High- or moderate-level evidence required studies to have no confounders and low risk of bias.
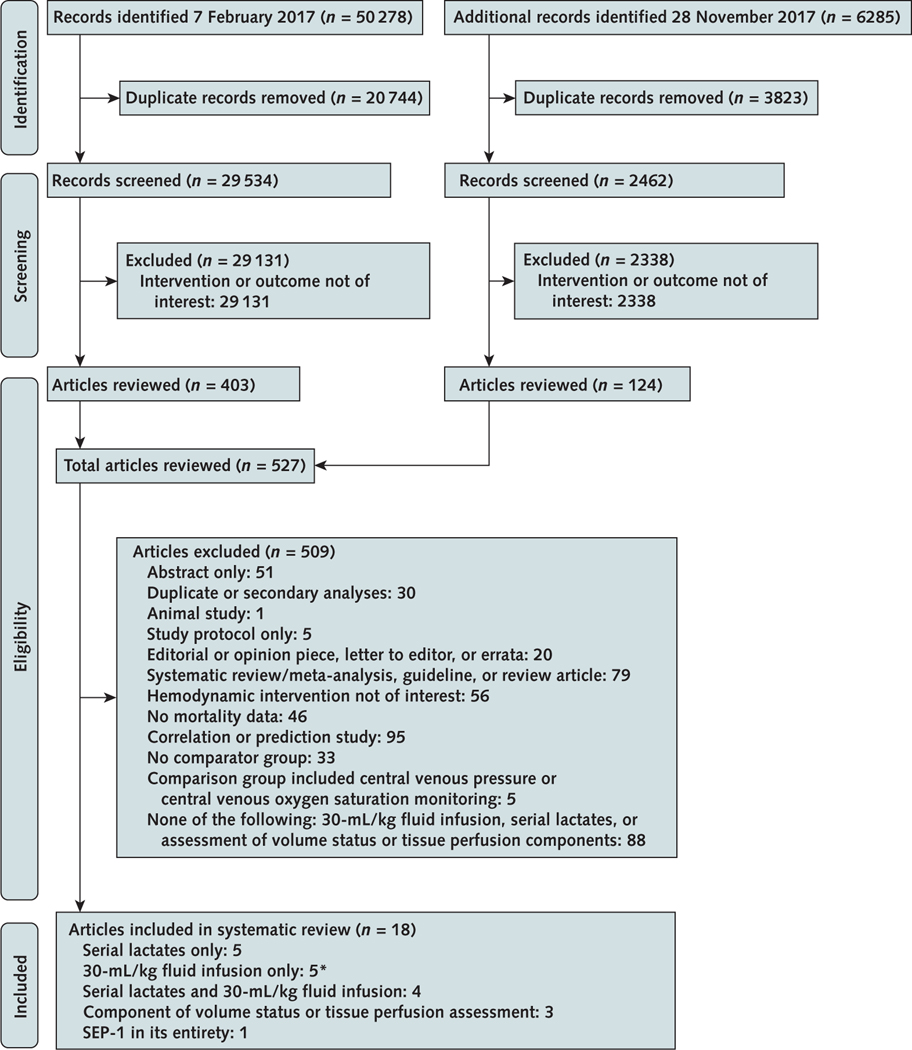
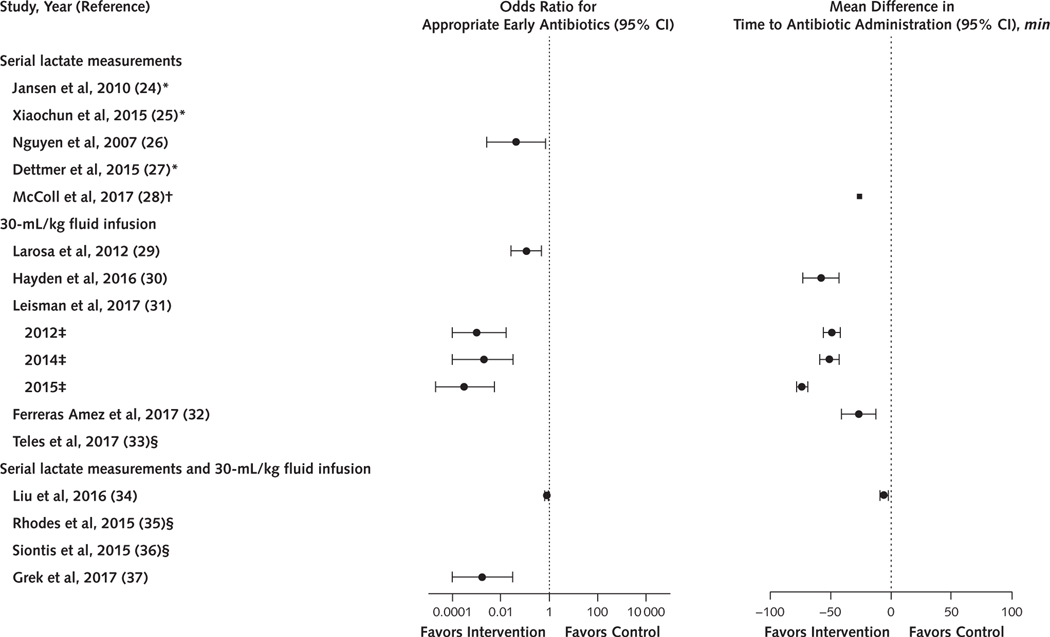
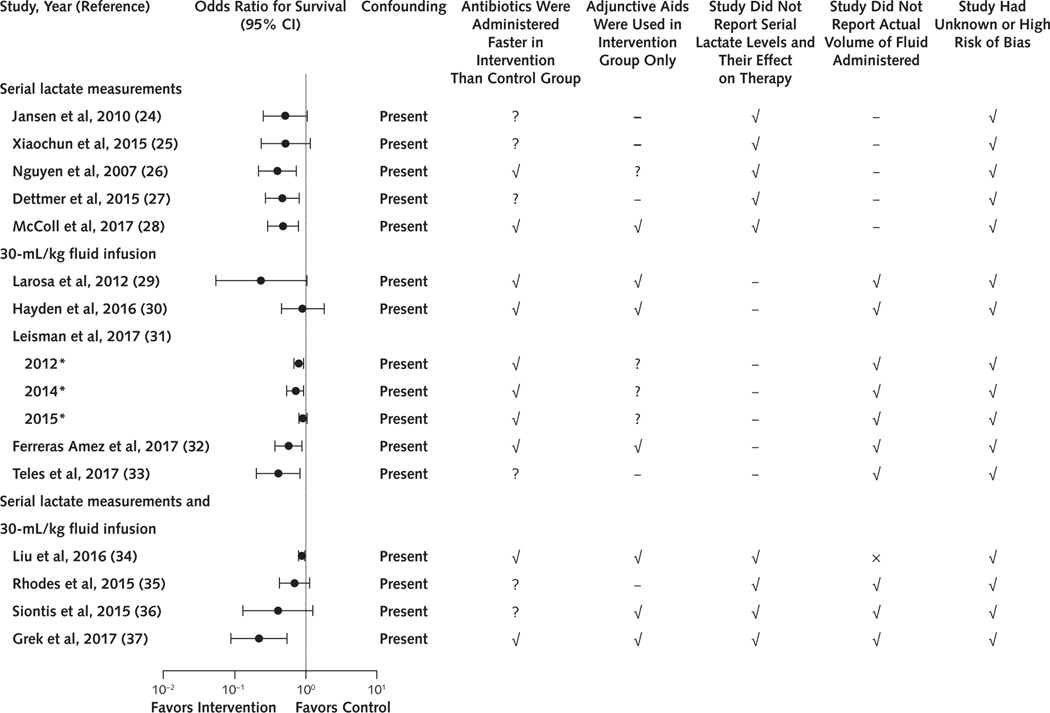
Data synthesis: Of 56 563 references, 20 studies (18 reports) met inclusion criteria. One single-center observational study reported lower in-hospital mortality after implementation of the SEP-1 bundle. Sixteen studies (2 randomized and 14 observational) reported increased survival with serial lactate measurements or 30-mL/kg fluid infusions. None of the 17 studies were free of confounders or at low risk of bias. In 3 randomized trials, fluid responsiveness testing did not alter survival.
Limitations: Few trials, poor-quality and confounded studies, and no studies (with survival outcomes) of the focused examination or bedside cardiovascular ultrasonography. Use of the 2015 version of SEP-1 and 2013 version of CMS evidence criteria, both of which were updated in 2017.
Conclusion: No high- or moderate-level evidence shows that SEP-1 or its hemodynamic interventions improve survival in adults with sepsis.
Primary funding source: National Institutes of Health. (PROSPERO: CRD42016052716).
Conflict of interest statement
Figures
Comment in
-
Treating Sepsis Is Complicated: Are Governmental Regulations for Sepsis Care Too Simplistic?Ann Intern Med. 2018 Apr 17;168(8):594-595. doi: 10.7326/M18-0290. Epub 2018 Feb 20. Ann Intern Med. 2018. PMID: 29459937 No abstract available.
-
Evidence Underpinning the Centers for Medicare & Medicaid Services' Severe Sepsis and Septic Shock Management Bundle (SEP-1).Ann Intern Med. 2018 Apr 17;168(8):610-612. doi: 10.7326/L18-0140. Ann Intern Med. 2018. PMID: 29543952 No abstract available.
-
Evidence Underpinning the Centers for Medicare & Medicaid Services' Severe Sepsis and Septic Shock Management Bundle (SEP-1).Ann Intern Med. 2018 Apr 17;168(8):609-610. doi: 10.7326/L18-0139. Ann Intern Med. 2018. PMID: 29543961 No abstract available.
References
-
- Centers for Medicare & Medicaid Services. CMS to improve quality of care during hospital inpatient stays. 4 August 2014. Accessed at www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2014-Fact-sheets-i... on 17 December 2017.
-
- The Joint Commission. Joint Commission Online. 2 September 2015. Accessed at www.jointcommission.org/assets/1/23/jconline_September_2_2015.pdf on 17 December 2017.
-
- National Health Foundation. NQF-endorsed voluntary consensus standards for hospital care measure information form. Measure set: sepsis. Version 5.0a. 2016. Accessed at www.nhfca.org/psf/resources/Updates1/SEP-1%20Measure%20Information%20For... on 17 December 2017.
-
- Version 5.2; Version 5.3, Version 5.4 The Joint Commission. Specifications Manual for National Hospital Inpatient Quality Measures. Accessed at www.jointcommission.org/specifications_manual_for_national_hospital_inpa... on 1 March 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous