

Experimental feasibility of spectral photon-counting computed tomography with two contrast agents for the detection of endoleaks following endovascular aortic repair
- PMID: 29460069
- PMCID: PMC6028848
- DOI: 10.1007/s00330-017-5252-7
Experimental feasibility of spectral photon-counting computed tomography with two contrast agents for the detection of endoleaks following endovascular aortic repair
Abstract
Objectives: After endovascular aortic repair (EVAR), discrimination of endoleaks and intra-aneurysmatic calcifications within the aneurysm often requires multiphase computed tomography (CT). Spectral photon-counting CT (SPCCT) in combination with a two-contrast agent injection protocol may provide reliable detection of endoleaks with a single CT acquisition.
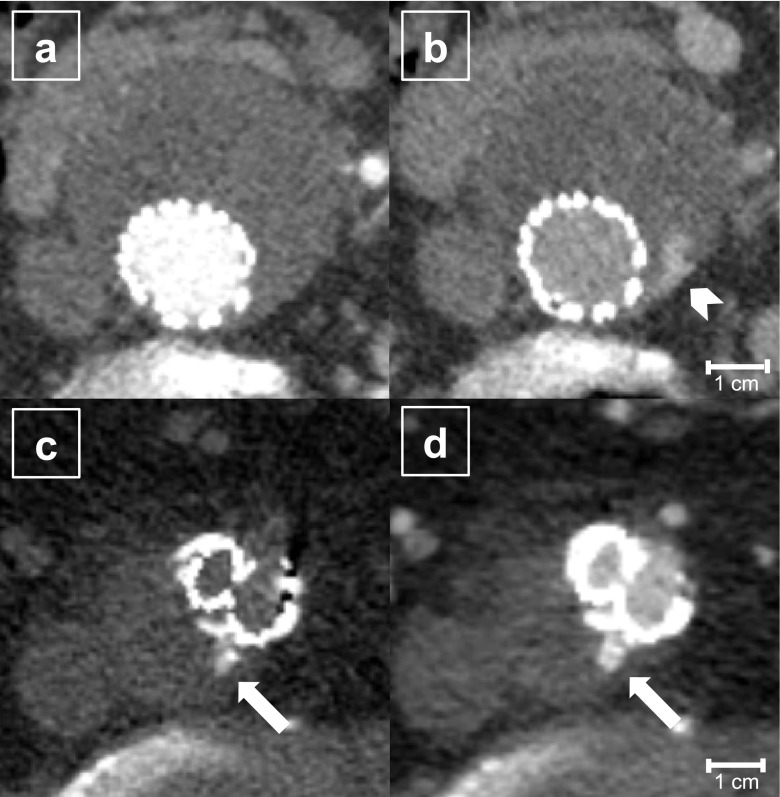
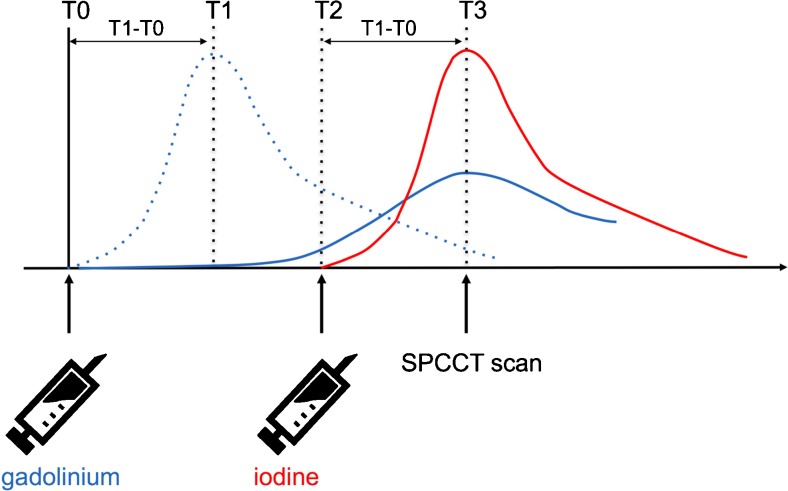
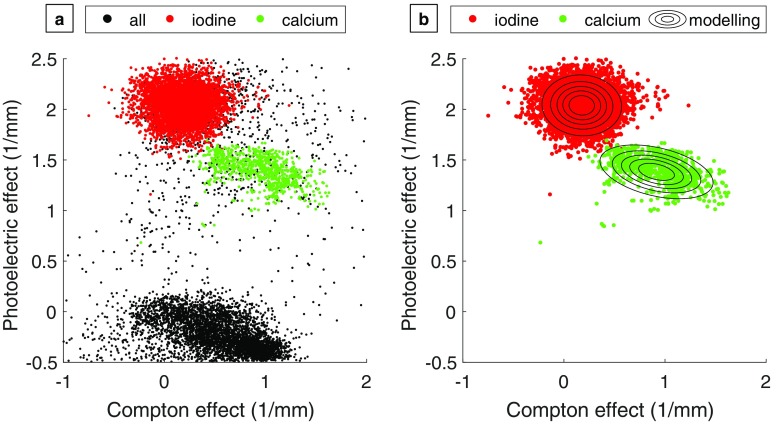
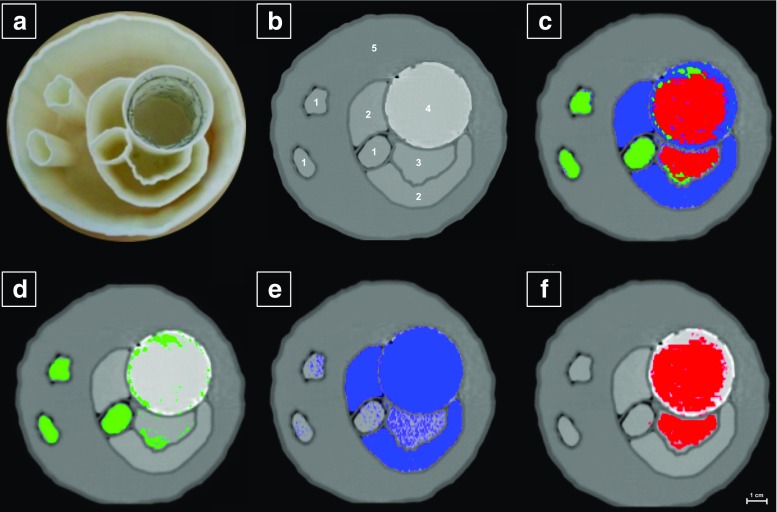
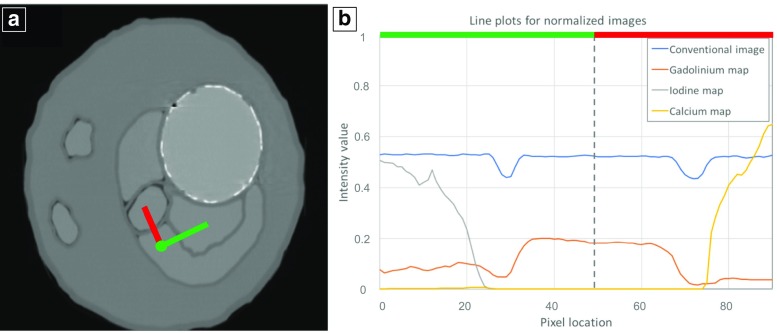
Methods: To evaluate the feasibility of SPCCT, the stent-lined compartment of an abdominal aortic aneurysm phantom was filled with a mixture of iodine and gadolinium mimicking enhanced blood. To represent endoleaks of different flow rates, the adjacent compartments contained either one of the contrast agents or calcium chloride to mimic intra-aneurysmatic calcifications. After data acquisition with a SPCCT prototype scanner with multi-energy bins, material decomposition was performed to generate iodine, gadolinium and calcium maps.
Results: In a conventional CT slice, Hounsfield units (HU) of the compartments were similar ranging from 147 to 168 HU. Material-specific maps differentiate the distributions within the compartments filled with iodine, gadolinium or calcium.
Conclusion: SPCCT may replace multiphase CT to detect endoleaks without sacrificing diagnostic accuracy. It is a unique feature of our method to capture endoleak dynamics and allow reliable distinction from intra-aneurysmatic calcifications in a single scan, thereby enabling a significant reduction of radiation exposure.
Key points: • SPCCT might enable advanced endoleak detection. • Material maps derived from SPCCT can differentiate iodine, gadolinium and calcium. • SPCCT may potentially reduce radiation burden for EVAR patients under post-interventional surveillance.
Keywords: Computed tomography; Endoleak; Gadolinium; Iodine; Photon counting.
Conflict of interest statement
Guarantor
The scientific guarantor of this publication is Peter B. Noël.
Conflict of interest
Heiner Daerr, Ewald Roessl and Roland Proksa are employees of Philips Healthcare. The remaining authors (Julia Dangelmaier, Daniel Bar-Ness, Daniela Muenzel, Salim Si-Mohamed, Sebastian Ehn, Alexander A. Fingerle, Melanie A. Kimm, Felix K. Kopp, Loic Boussel, Franz Pfeiffer, Ernst J. Rummeny, Philippe Douek and Peter B. Noël) declare no conflict of interest.
Statistics and biometry
No complex statistical methods were necessary for this paper.
Informed consent
Written informed consent was not required for this study because the study was phantom-based.
Ethical approval
Institutional review board approval was not required because the study was phantom-based.
Methodology
• prospective
• experimental
• performed at one institution
Figures
References
-
- Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease): endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. Circulation. 2006;113:e463–e654. doi: 10.1161/CIRCULATIONAHA.106.174526. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
