

Time Is Cerebellum
- PMID: 29460203
- PMCID: PMC6028834
- DOI: 10.1007/s12311-018-0925-6
Time Is Cerebellum
Abstract
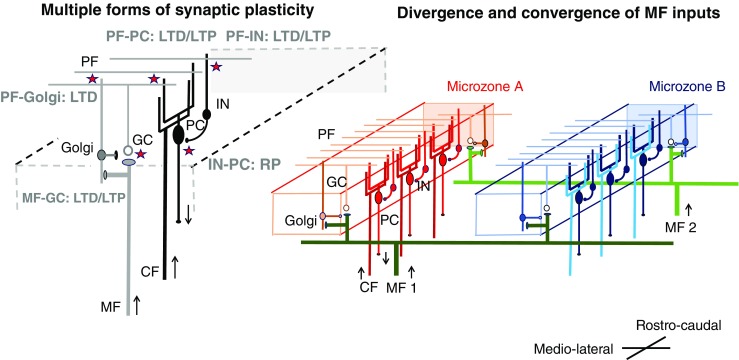
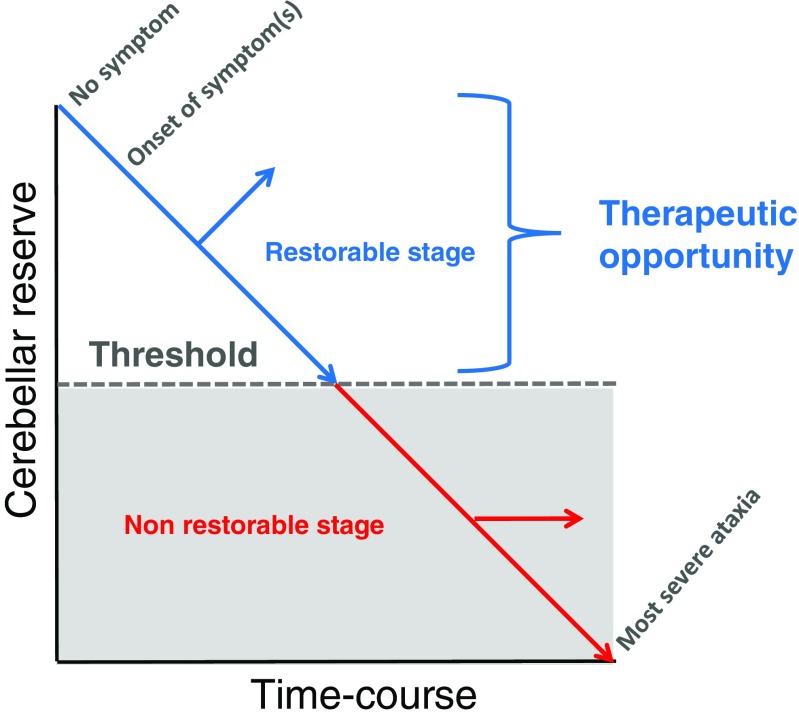
The cerebellum characteristically has the capacity to compensate for and restore lost functions. These compensatory/restorative properties are explained by an abundant synaptic plasticity and the convergence of multimodal central and peripheral signals. In addition, extra-cerebellar structures contribute also to the recovery after a cerebellar injury. Clinically, some patients show remarkable improvement of severe ataxic symptoms associated with trauma, stroke, metabolism, or immune-mediated cerebellar ataxia (IMCA, e.g., multiple sclerosis, paraneoplastic cerebellar degeneration, gluten ataxia, anti-GAD65 antibody-associated cerebellar ataxia). However, extension of a cerebellar lesion can impact upon the fourth ventricle or the brainstem, either by direct or indirect mechanisms, leading to serious complications. Moreover, cerebellar reserve itself is affected by advanced cell loss and, at some point of disease progression, deficits become irreversible. Such phase transition from a treatable/restorable state (the reserve is still sufficient) to an untreatable state (the reserve is severely affected) is a loss of therapeutic opportunity, highlighting the need for early treatment during the restorable stage. Based on the motto of "Time is Brain," a warning that stresses the importance of early therapeutic intervention in ischemic diseases, we propose "Time is Cerebellum" as a principle in the management of patients with cerebellar diseases, especially immune ataxias whose complexity often delay the therapeutic intervention. Indeed, this concept should not be restricted to ischemic cerebellar diseases. We argue that every effort should be made to reduce the diagnostic delay and to initiate early therapy to avoid the risk of transition from a treatable state to an irreversible condition and an associated accumulation of disability. The myriad of disorders affecting the cerebellum is a challenging factor that may contribute to irreversible disability if the window of therapeutic opportunity is missed.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Hacke Werner, Kaste Markku, Bluhmki Erich, Brozman Miroslav, Dávalos Antoni, Guidetti Donata, Larrue Vincent, Lees Kennedy R., Medeghri Zakaria, Machnig Thomas, Schneider Dietmar, von Kummer Rüdiger, Wahlgren Nils, Toni Danilo. Thrombolysis with Alteplase 3 to 4.5 Hours after Acute Ischemic Stroke. New England Journal of Medicine. 2008;359(13):1317–1329. doi: 10.1056/NEJMoa0804656. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
