

Impact of the scale-up of piped water on urogenital schistosomiasis infection in rural South Africa
- PMID: 29460779
- PMCID: PMC5819946
- DOI: 10.7554/eLife.33065
Impact of the scale-up of piped water on urogenital schistosomiasis infection in rural South Africa
Abstract
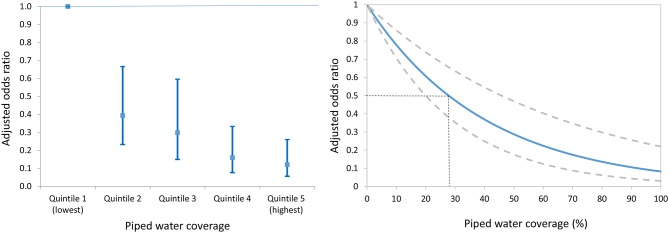
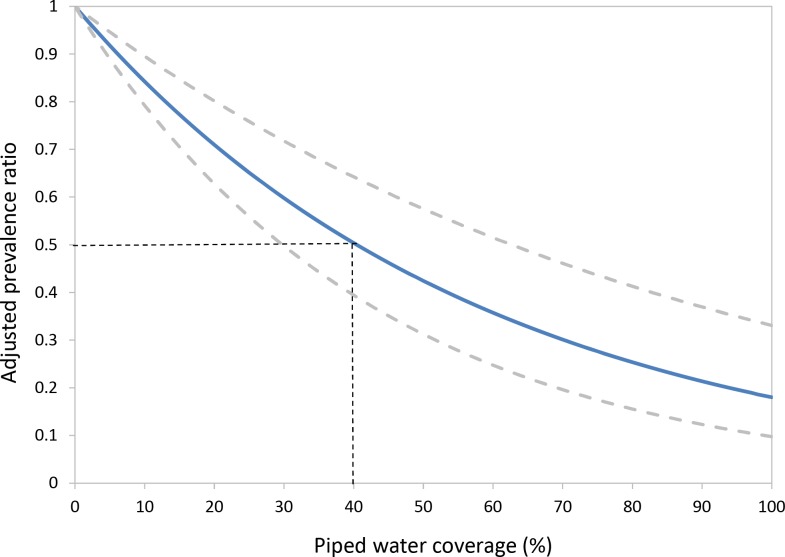
Recent work has estimated that sub-Saharan Africa could lose US$3.5 billion of economic productivity every year as a result of schistosomiasis and soil-transmitted helminthiasis. One of the main interventions to control schistosomiasis is the provision of safe water to limit the contact with infected water bodies and break the cycle of transmission. To date, a rigorous quantification of the impact of safe water supplies on schistosomiasis is lacking. Using data from one of Africa's largest population-based cohorts, we establish the impact of the scale-up of piped water in a typical rural South African population over a seven-year time horizon. High coverage of piped water in the community decreased a child's risk of urogenital schistosomiasis infection eight-fold (adjusted odds ratio = 0.12, 95% CI 0.06-0.26, p<0.001). The provision of safe water could drive levels of urogenital schistosomiasis infection to low levels of endemicity in rural African settings.
Keywords: Africa; epidemiology; global health; human; infectious disease; microbiology; sanitation; spatial analysis; urogenital schistosomiasis; water.
© 2018, Tanser et al.
Conflict of interest statement
FT, DA, AV, TB, CA No competing interests declared
Figures
References
-
- Al-Waleedi AA, El-Nimr NA, Hasab AA, Bassiouny HK, Al-Shibani LA. Urinary schistosomiasis among schoolchildren in Yemen: prevalence, risk factors, and the effect of a chemotherapeutic intervention. The Journal of the Egyptian Public Health Association. 2013;88:130–136. doi: 10.1097/01.EPX.0000441277.96615.96. - DOI - PubMed
-
- Angrist JD, Imbens GW, Rubin DB. Identification of causal effects using instrumental variables. Journal of the American Statistical Association. 1996;91:444–455. doi: 10.1080/01621459.1996.10476902. - DOI
-
- Appleton CC, Kvalsvig JD. A school-based helminth control programme successfully implemented in KwaZulu-Natal. Southern African Journal of Epidemiology and Infection. 2006;21:55–67. doi: 10.1080/10158782.2006.11441265. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
