

Clinical implications of PTEN loss in prostate cancer
- PMID: 29460925
- PMCID: PMC7472658
- DOI: 10.1038/nrurol.2018.9
Clinical implications of PTEN loss in prostate cancer
Abstract
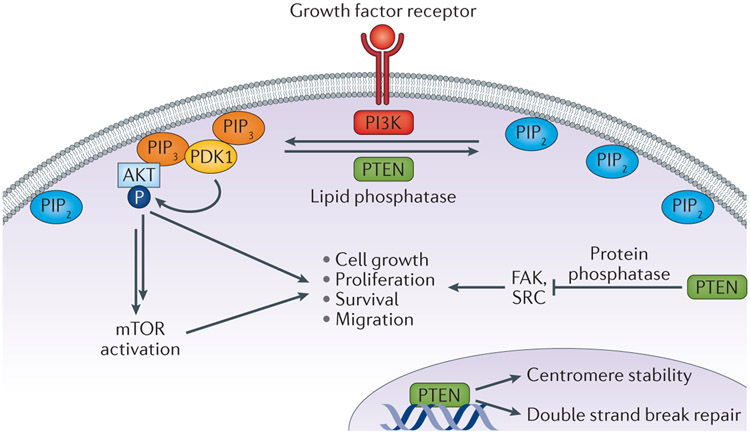
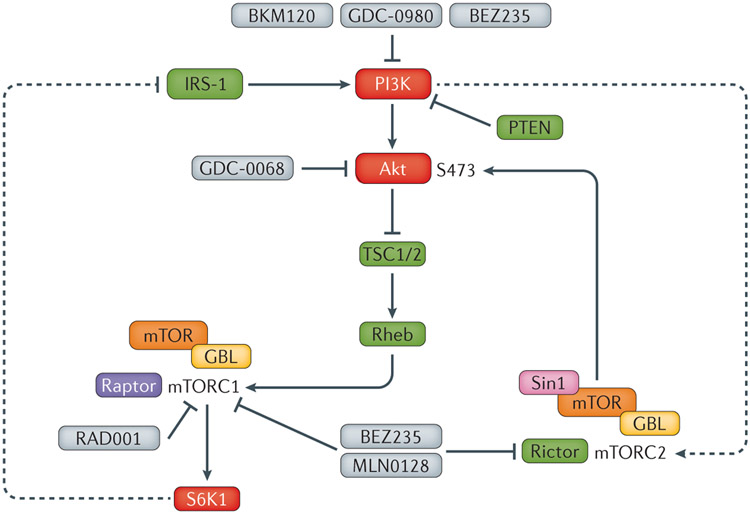
Genomic aberrations of the PTEN tumour suppressor gene are among the most common in prostate cancer. Inactivation of PTEN by deletion or mutation is identified in ∼20% of primary prostate tumour samples at radical prostatectomy and in as many as 50% of castration-resistant tumours. Loss of phosphatase and tensin homologue (PTEN) function leads to activation of the PI3K-AKT (phosphoinositide 3-kinase-RAC-alpha serine/threonine-protein kinase) pathway and is strongly associated with adverse oncological outcomes, making PTEN a potentially useful genomic marker to distinguish indolent from aggressive disease in patients with clinically localized tumours. At the other end of the disease spectrum, therapeutic compounds targeting nodes in the PI3K-AKT-mTOR (mechanistic target of rapamycin) signalling pathway are being tested in clinical trials for patients with metastatic castration-resistant prostate cancer. Knowledge of PTEN status might be helpful to identify patients who are more likely to benefit from these therapies. To enable the use of PTEN status as a prognostic and predictive biomarker, analytically validated assays have been developed for reliable and reproducible detection of PTEN loss in tumour tissue and in blood liquid biopsies. The use of clinical-grade assays in tumour tissue has shown a robust correlation between loss of PTEN and its protein as well as a strong association between PTEN loss and adverse pathological features and oncological outcomes. In advanced disease, assessing PTEN status in liquid biopsies shows promise in predicting response to targeted therapy. Finally, studies have shown that PTEN might have additional functions that are independent of the PI3K-AKT pathway, including those affecting tumour growth through modulation of the immune response and tumour microenvironment.
Conflict of interest statement
Competing interests statement
T.L.L. has received research support from Ventana Medical Systems. D.M.B. has received financial support from Myriad Genetics and Metamark Genetics.
Figures

References
-
- Maehama T & Dixon JE The tumor suppressor, PTEN/MMAC1, dephosphorylates the lipid second messenger, phosphatidylinositol 3,4,5-trisphosphate. J Biol Chem 273, 13375–13378 (1998). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
