

Long-Term Oncologic Outcomes, Opioid Use, and Complications after Esophageal Cancer Surgery
- PMID: 29463006
- PMCID: PMC5852449
- DOI: 10.3390/jcm7020033
Long-Term Oncologic Outcomes, Opioid Use, and Complications after Esophageal Cancer Surgery
Abstract
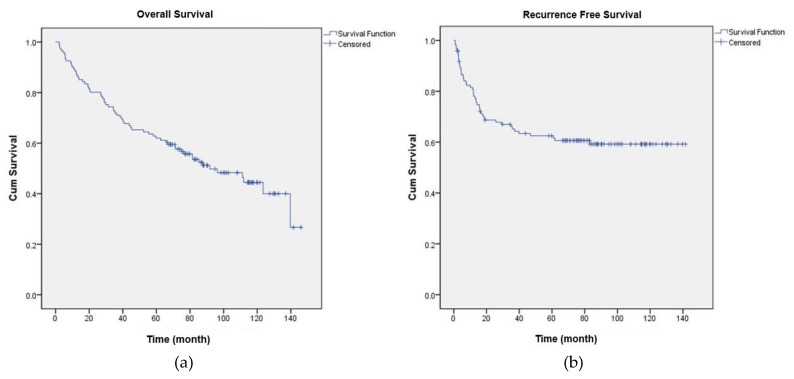
Effective and adequate opioid use and prevention of postoperative complications are important for enhanced recovery after surgery. We examined the effects of postoperative opioid use and postoperative complications on overall survival and recurrence-free survival after esophageal cancer surgery. This retrospective cohort study analyzed the records of patients diagnosed with esophageal cancer who underwent the Ivor Lewis operation between January 2005 and December 2011. We collected data on total opioid use for 8 days postoperatively, as well as information on postoperative complications (Clavien-Dindo classification). One hundred and twenty-one patients were included in the final analysis. Total opioid use was not significantly associated with overall survival (p = 0.520) and recurrence-free survival (p = 0.818). In contrast, the hazard ratio of postoperative overall survival was significantly higher with respect to Clavien-Dindo classification 1-2 (hazard ratio: 2.009, p = 0.046), 3a-3b (hazard ratio: 5.759, p < 0.001), and 4a-5 (hazard ratio: 3.982, p = 0.020) complications compared to no complications. Additionally, the hazard ratio of the recurrence-free survival was significantly higher in class 1-2 complications (hazard ratio: 2.336, p = 0.028) compared to none. Our study demonstrates that postoperative opioid use is not associated with survival and recurrence-free survival after esophageal cancer surgery, while postoperative complications may increase the hazard ratio for survival and recurrence-free survival.
Keywords: analgesia; anesthesia; esophageal neoplasms; esophagus.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Worni M., Castleberry A.W., Gloor B., Pietrobon R., Haney J.C., D’Amico T.A., Akushevich I., Berry M.F. Trends and outcomes in the use of surgery and radiation for the treatment of locally advanced esophageal cancer: A propensity score adjusted analysis of the surveillance, epidemiology, and end results registry from 1998 to 2008. Dis. Esophagus. 2014;27:662–669. doi: 10.1111/dote.12123. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
