

Next-generation, personalised, model-based critical care medicine: a state-of-the art review of in silico virtual patient models, methods, and cohorts, and how to validation them
- PMID: 29463246
- PMCID: PMC5819676
- DOI: 10.1186/s12938-018-0455-y
Next-generation, personalised, model-based critical care medicine: a state-of-the art review of in silico virtual patient models, methods, and cohorts, and how to validation them
Abstract
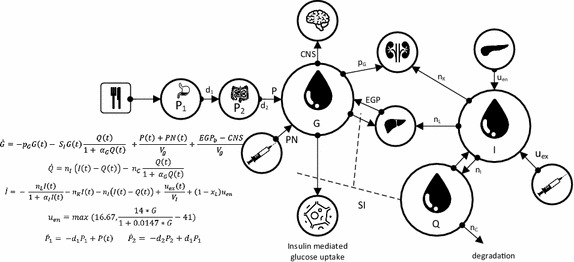
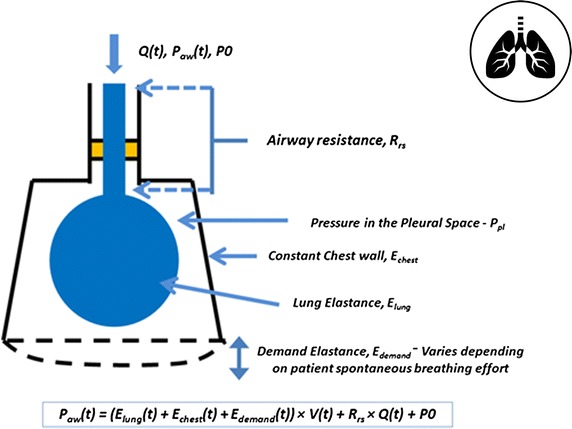
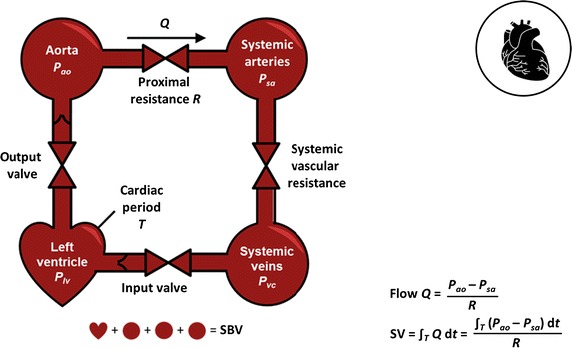
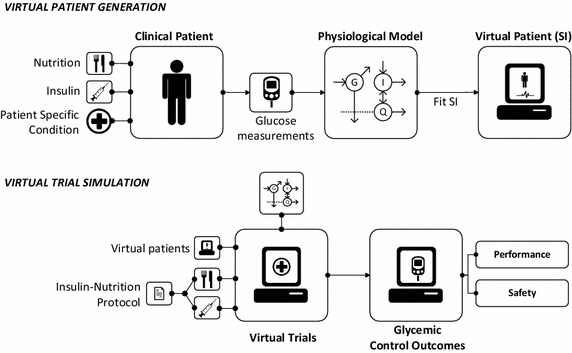
Critical care, like many healthcare areas, is under a dual assault from significantly increasing demographic and economic pressures. Intensive care unit (ICU) patients are highly variable in response to treatment, and increasingly aging populations mean ICUs are under increasing demand and their cohorts are increasingly ill. Equally, patient expectations are growing, while the economic ability to deliver care to all is declining. Better, more productive care is thus the big challenge. One means to that end is personalised care designed to manage the significant inter- and intra-patient variability that makes the ICU patient difficult. Thus, moving from current "one size fits all" protocolised care to adaptive, model-based "one method fits all" personalised care could deliver the required step change in the quality, and simultaneously the productivity and cost, of care. Computer models of human physiology are a unique tool to personalise care, as they can couple clinical data with mathematical methods to create subject-specific models and virtual patients to design new, personalised and more optimal protocols, as well as to guide care in real-time. They rely on identifying time varying patient-specific parameters in the model that capture inter- and intra-patient variability, the difference between patients and the evolution of patient condition. Properly validated, virtual patients represent the real patients, and can be used in silico to test different protocols or interventions, or in real-time to guide care. Hence, the underlying models and methods create the foundation for next generation care, as well as a tool for safely and rapidly developing personalised treatment protocols over large virtual cohorts using virtual trials. This review examines the models and methods used to create virtual patients. Specifically, it presents the models types and structures used and the data required. It then covers how to validate the resulting virtual patients and trials, and how these virtual trials can help design and optimise clinical trial. Links between these models and higher order, more complex physiome models are also discussed. In each section, it explores the progress reported up to date, especially on core ICU therapies in glycemic, circulatory and mechanical ventilation management, where high cost and frequency of occurrence provide a significant opportunity for model-based methods to have measurable clinical and economic impact. The outcomes are readily generalised to other areas of medical care.
Figures
References
-
- Halpern NA. Can the costs of critical care be controlled? Curr Opin Crit Care. 2009;15(6):591–596. - PubMed
-
- Shorr AF. An update on cost-effectiveness analysis in critical care. Curr Opin Crit Care. 2002;8(4):337–343. - PubMed
-
- Halpern SD. ICU capacity strain and the quality and allocation of critical care. Curr Opin Crit Care. 2011;17(6):648–657. - PubMed
-
- van Exel J, Baker R, Mason H, Donaldson C, Brouwer W, EuroVa QT. Public views on principles for health care priority setting: findings of a European cross-country study using Q methodology. Soc Sci Med. 2015;126:128–137. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
