

Sepsis-Induced T Cell Immunoparalysis: The Ins and Outs of Impaired T Cell Immunity
- PMID: 29463691
- PMCID: PMC5826615
- DOI: 10.4049/jimmunol.1701618
Sepsis-Induced T Cell Immunoparalysis: The Ins and Outs of Impaired T Cell Immunity
Abstract
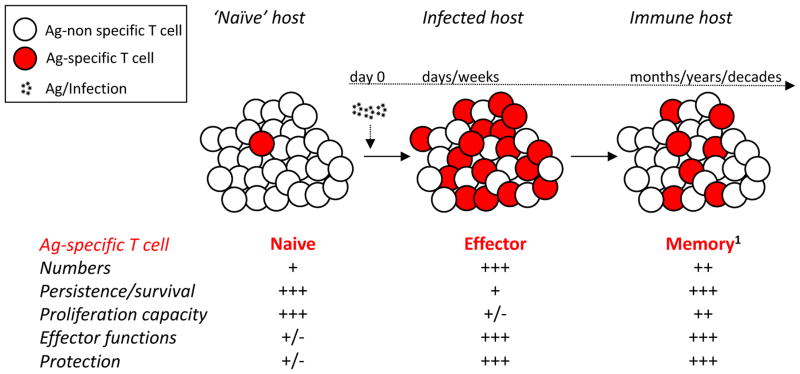
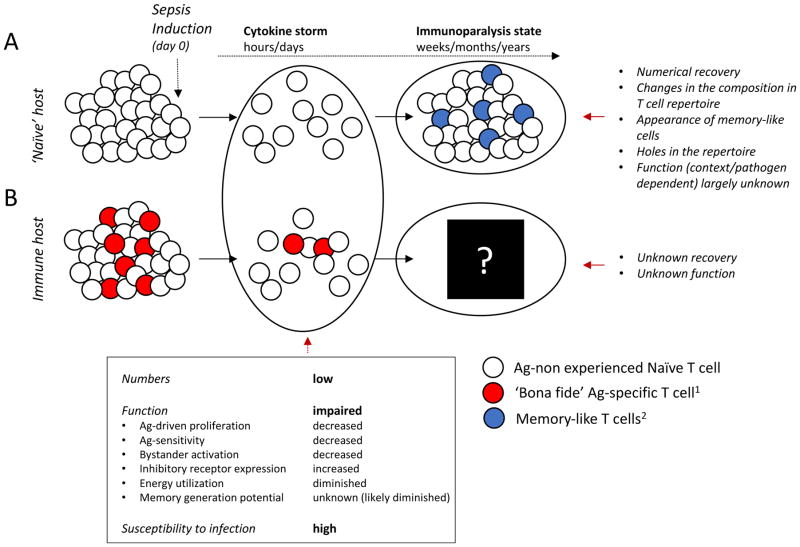
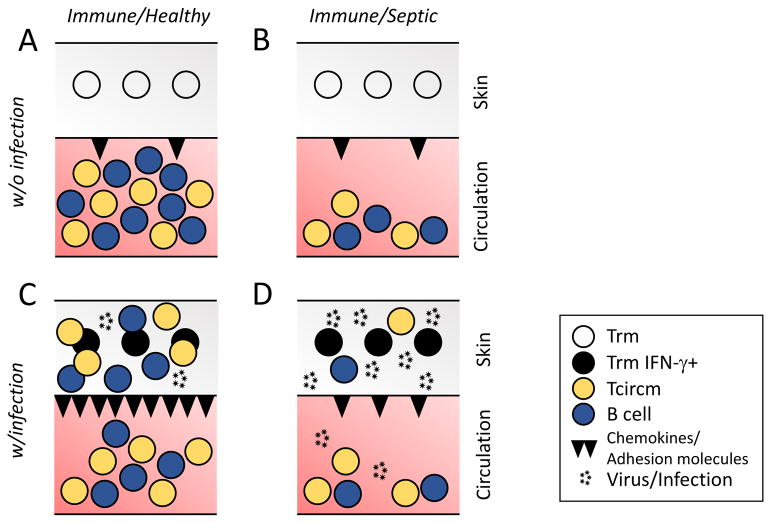
Sepsis results in a deluge of pro- and anti-inflammatory cytokines, leading to lymphopenia and chronic immunoparalysis. Sepsis-induced long-lasting immunoparalysis is defined, in part, by impaired CD4 and CD8 αβ T cell responses in the postseptic environment. The dysfunction in T cell immunity affects naive, effector, and memory T cells and is not restricted to classical αβ T cells. Although sepsis-induced severe and transient lymphopenia is a contributory factor to diminished T cell immunity, T cell-intrinsic and -extrinsic factors/mechanisms also contribute to impaired T cell function. In this review, we summarize the current knowledge of how sepsis quantitatively and qualitatively impairs CD4 and CD8 T cell immunity of classical and nonclassical T cell subsets and discuss current therapeutic approaches being developed to boost the recovery of T cell immunity postsepsis induction.
Copyright © 2018 by The American Association of Immunologists, Inc.
Figures
References
-
- CDC. Sepsis: Data & Reports. Center for Disease Control and Prevention; 2017. https://www.cdc.gov/sepsis/datareports/index.html.
-
- Dombrovskiy VY, Martin AA, Sunderram J, Paz HL. Rapid increase in hospitalization and mortality rates for severe sepsis in the United States: A trend analysis from 1993 to 2003*. Crit Care Med. 2007;35:1244–50. - PubMed
-
- Gaieski DF, Edwards JM, Kallan MJ, Carr BG. Benchmarking the Incidence and Mortality of Severe Sepsis in the United States*. Crit Care Med. 2013;41:1167–74. - PubMed
-
- Kutza AST, Muhl E, Hackstein H, Kirchner H, Bein G. High Incidence of Active Cytomegalovirus Infection Among Septic Patients. Clin Infect Dis. 1998;26:1076–82. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
