

Acid and the basis for cellular plasticity and reprogramming in gastric repair and cancer
- PMID: 29463907
- PMCID: PMC6016373
- DOI: 10.1038/nrgastro.2018.5
Acid and the basis for cellular plasticity and reprogramming in gastric repair and cancer
Abstract
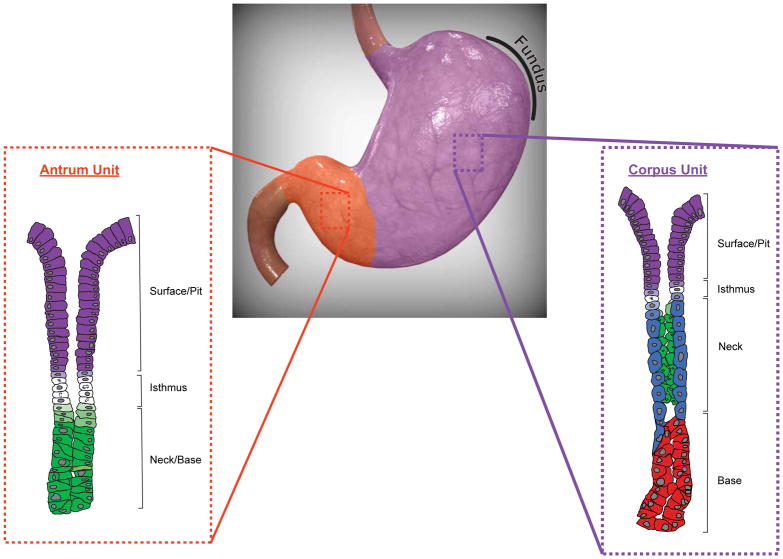
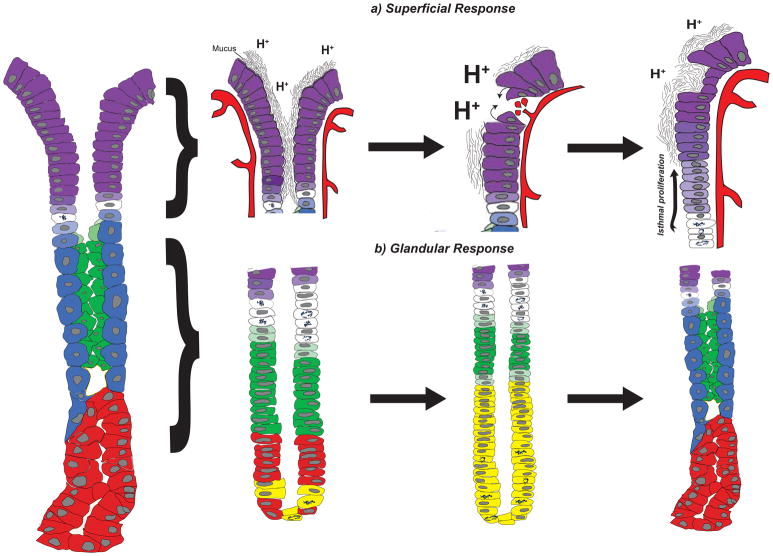
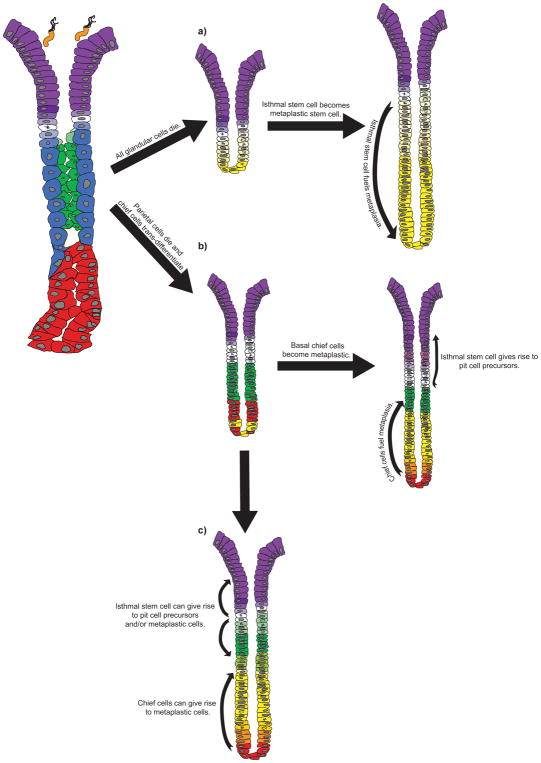
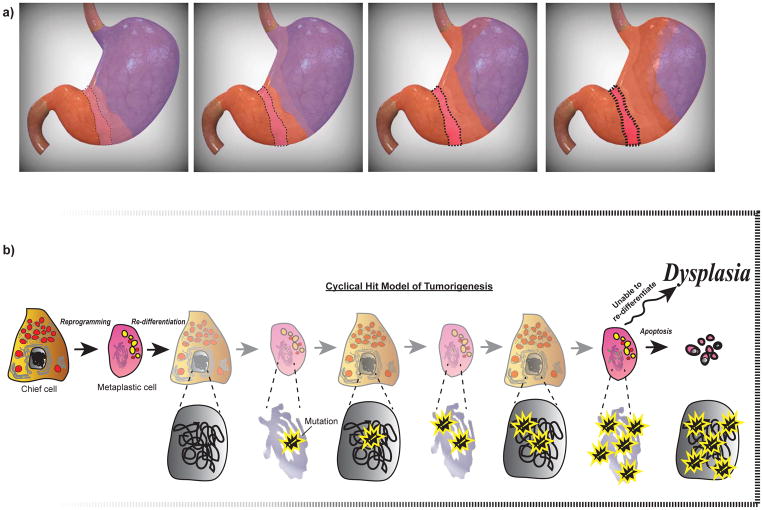
Subjected to countless daily injuries, the stomach still functions as a remarkably efficient digestive organ and microbial filter. In this Review, we follow the lead of the earliest gastroenterologists who were fascinated by the antiseptic and digestive powers of gastric secretions. We propose that it is easiest to understand how the stomach responds to injury by stressing the central role of the most important gastric secretion, acid. The stomach follows two basic patterns of adaptation. The superficial response is a pattern whereby the surface epithelial cells migrate and rapidly proliferate to repair erosions induced by acid or other irritants. The stomach can also adapt through a glandular response when the source of acid is lost or compromised (that is, the process of oxyntic atrophy). We primarily review the mechanisms governing the glandular response, which is characterized by a metaplastic change in cellular differentiation known as spasmolytic polypeptide-expressing metaplasia (SPEM). We propose that the stomach, like other organs, exhibits marked cellular plasticity: the glandular response involves reprogramming mature cells to serve as auxiliary stem cells that replace lost cells. Unfortunately, such plasticity might mean that the gastric epithelium undergoes cycles of differentiation and de-differentiation that increase the risk of accumulating cancer-predisposing mutations.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- De Fourcroy AF. Élémens d’Histoire Naturelle et de Chimie. Cuchet; Paris: 1791. pp. 357–62.
-
- Spallanzani L. Dissertations Relative to the Natural History of Animals and Vegetables. Vol. 1. J. Murray; London: 1789. This was one of the first treatises focusing on the stomach and its role in digestion.
-
- Ferlay J, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–386. - PubMed
-
- Colquhoun A, et al. Global patterns of cardia and non-cardia gastric cancer incidence in 2012. Gut. 2015;64:1881–1888. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
