

Impact of co-administration of oxycodone and smoked cannabis on analgesia and abuse liability
- PMID: 29463913
- PMCID: PMC6098090
- DOI: 10.1038/s41386-018-0011-2
Impact of co-administration of oxycodone and smoked cannabis on analgesia and abuse liability
Abstract
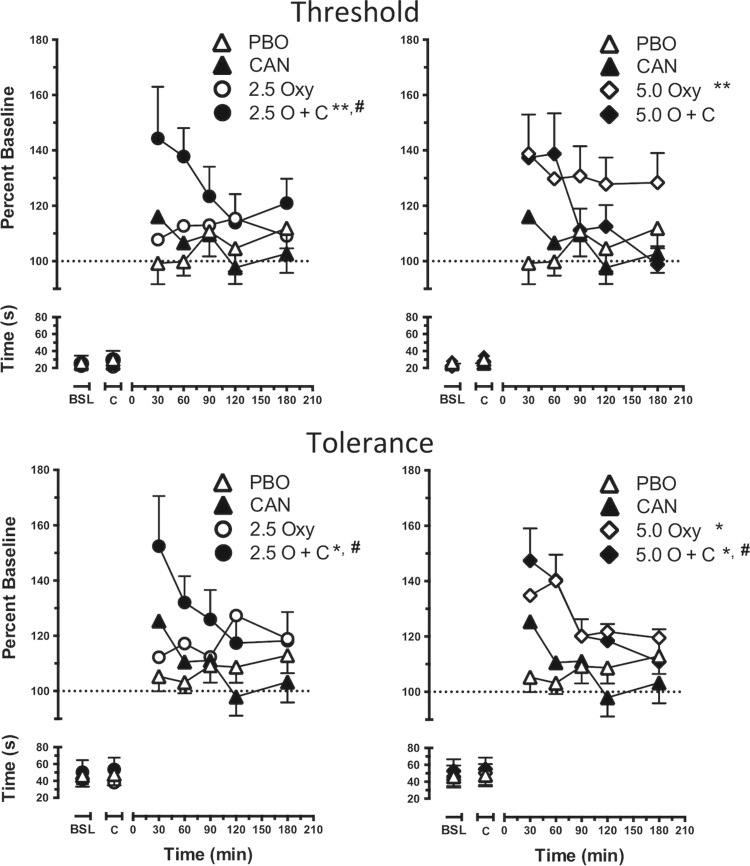
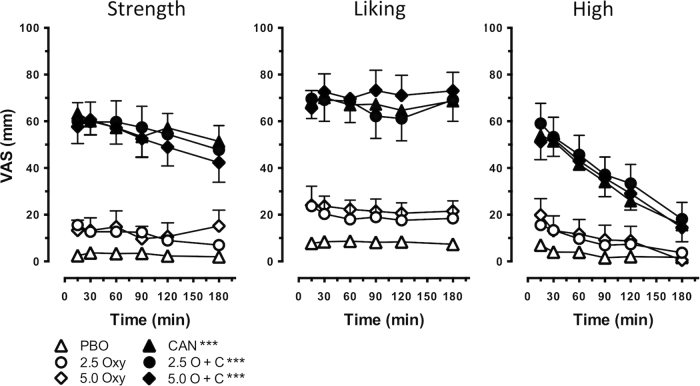
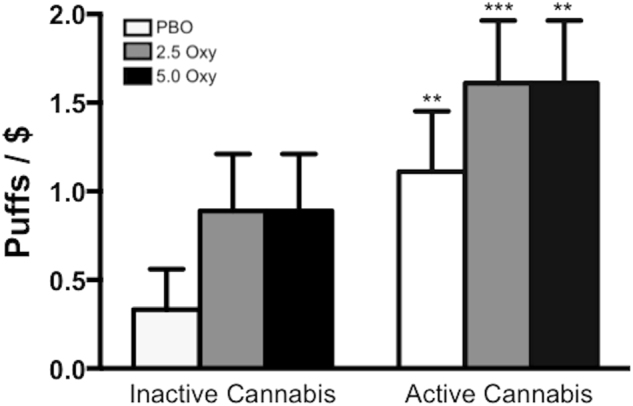
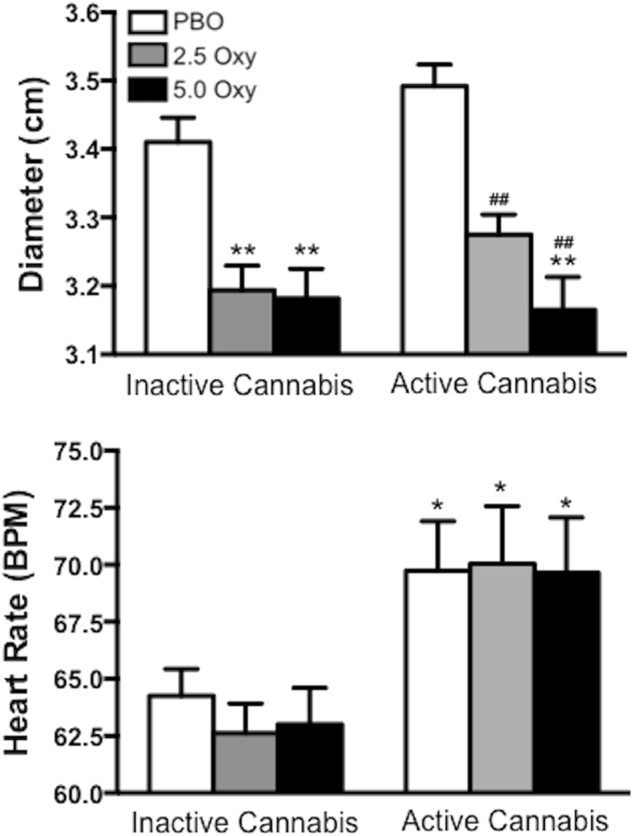
Cannabinoids combined with opioids produce synergistic antinociceptive effects, decreasing the lowest effective antinociceptive opioid dose (i.e., opioid-sparing effects) in laboratory animals. Although pain patients report greater analgesia when cannabis is used with opioids, no placebo-controlled studies have assessed the direct effects of opioids combined with cannabis in humans or the impact of the combination on abuse liability. This double-blind, placebo-controlled, within-subject study determined if cannabis enhances the analgesic effects of low dose oxycodone using a validated experimental model of pain and its effects on abuse liability. Healthy cannabis smokers (N = 18) were administered oxycodone (0, 2.5, and 5.0 mg, PO) with smoked cannabis (0.0, 5.6% Δ9 tetrahydrocannabinol [THC]) and analgesia was assessed using the Cold-Pressor Test (CPT). Participants immersed their hand in cold water (4 °C); times to report pain (pain threshold) and withdraw the hand from the water (pain tolerance) were recorded. Abuse-related effects were measured and effects of oxycodone on cannabis self-administration were determined. Alone, 5.0 mg oxycodone increased pain threshold and tolerance (p ≤ 0.05). Although active cannabis and 2.5 mg oxycodone alone failed to elicit analgesia, combined they increased pain threshold and tolerance (p ≤ 0.05). Oxycodone did not increase subjective ratings associated with cannabis abuse, nor did it increase cannabis self-administration. However, the combination of 2.5 mg oxycodone and active cannabis produced small, yet significant, increases in oxycodone abuse liability (p ≤ 0.05). Cannabis enhances the analgesic effects of sub-threshold oxycodone, suggesting synergy, without increases in cannabis's abuse liability. These findings support future research into the therapeutic use of opioid-cannabinoid combinations for pain.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Considering abuse liability and neurocognitive effects of cannabis and cannabis-derived products when assessing analgesic efficacy: a comprehensive review of randomized-controlled studies.Am J Drug Alcohol Abuse. 2019;45(6):580-595. doi: 10.1080/00952990.2019.1669628. Epub 2019 Nov 5. Am J Drug Alcohol Abuse. 2019. PMID: 31687845 Free PMC article. Review.
-
Sex-dependent effects of cannabis-induced analgesia.Drug Alcohol Depend. 2016 Oct 1;167:112-20. doi: 10.1016/j.drugalcdep.2016.08.001. Epub 2016 Aug 5. Drug Alcohol Depend. 2016. PMID: 27522535 Free PMC article. Clinical Trial.
-
Comparison of the analgesic effects of dronabinol and smoked marijuana in daily marijuana smokers.Neuropsychopharmacology. 2013 Sep;38(10):1984-92. doi: 10.1038/npp.2013.97. Epub 2013 Apr 22. Neuropsychopharmacology. 2013. PMID: 23609132 Free PMC article. Clinical Trial.
-
Cannabinoid modulation of opioid analgesia and subjective drug effects in healthy humans.Psychopharmacology (Berl). 2019 Nov;236(11):3341-3352. doi: 10.1007/s00213-019-05293-1. Epub 2019 Jun 15. Psychopharmacology (Berl). 2019. PMID: 31201479 Free PMC article. Clinical Trial.
-
Synergistic interactions between cannabinoid and opioid analgesics.Life Sci. 2004 Jan 30;74(11):1317-24. doi: 10.1016/j.lfs.2003.09.038. Life Sci. 2004. PMID: 14706563 Review.
Cited by
-
Potential Pharmacokinetic Drug-Drug Interactions between Cannabinoids and Drugs Used for Chronic Pain.Biomed Res Int. 2020 Aug 13;2020:3902740. doi: 10.1155/2020/3902740. eCollection 2020. Biomed Res Int. 2020. PMID: 32855964 Free PMC article. Review.
-
Substituting Cannabidiol for Opioids and Pain Medications Among Individuals With Fibromyalgia: A Large Online Survey.J Pain. 2021 Nov;22(11):1418-1428. doi: 10.1016/j.jpain.2021.04.011. Epub 2021 May 13. J Pain. 2021. PMID: 33992787 Free PMC article.
-
Considering abuse liability and neurocognitive effects of cannabis and cannabis-derived products when assessing analgesic efficacy: a comprehensive review of randomized-controlled studies.Am J Drug Alcohol Abuse. 2019;45(6):580-595. doi: 10.1080/00952990.2019.1669628. Epub 2019 Nov 5. Am J Drug Alcohol Abuse. 2019. PMID: 31687845 Free PMC article. Review.
-
Real-Time Monitoring of Cannabis and Prescription Opioid Co-Use Patterns, Analgesic Effectiveness, and the Opioid-Sparing Effect of Cannabis in Individuals With Chronic Pain.J Pain. 2022 Nov;23(11):1799-1810. doi: 10.1016/j.jpain.2022.06.009. Epub 2022 Jul 8. J Pain. 2022. PMID: 35817255 Free PMC article.
-
Δ9-tetrahydrocannabinol attenuates oxycodone self-administration under extended access conditions.Neuropharmacology. 2019 Jun;151:127-135. doi: 10.1016/j.neuropharm.2019.04.010. Epub 2019 Apr 11. Neuropharmacology. 2019. PMID: 30980837 Free PMC article.
References
-
- National Institute on Drug Abuse (2017). Overdose Death Rates. at https://www.drugabuse.gov/related-topics/trends-statistics/overdose-deat....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
