

Improved Cuff Technique and Intraoperative Detection of Vascular Complications for Hind Limb Transplantation in Mice
- PMID: 29464206
- PMCID: PMC5811274
- DOI: 10.1097/TXD.0000000000000756
Improved Cuff Technique and Intraoperative Detection of Vascular Complications for Hind Limb Transplantation in Mice
Abstract
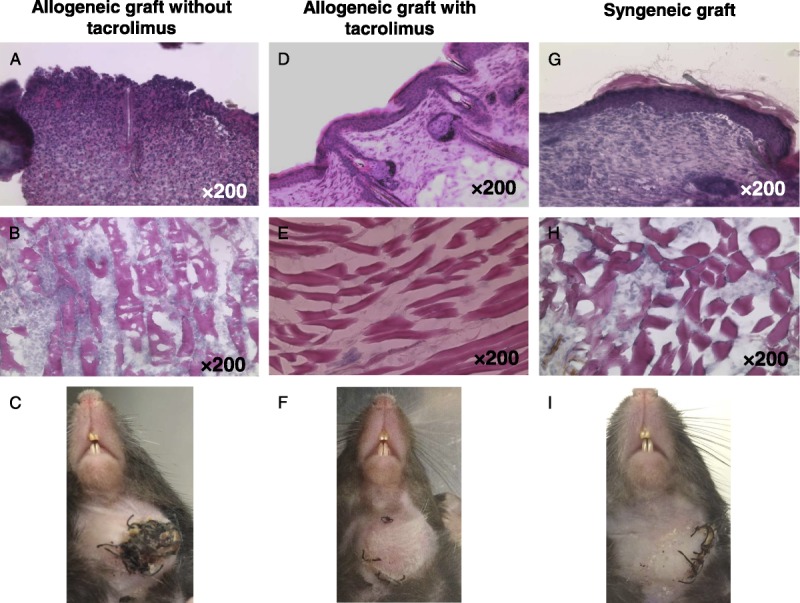
Background: Vascularized composite tissue allotransplantation (VCA) from a cadaveric donor has now become a clinical reality and the treatment modality of choice for patients with devastating injuries, deformities, and complex tissue defects. However, many VCA patients experience severe toxicities due to the strong immunosuppression required secondary to high antigenicity of the grafts. To improve immunosuppressive protocols for VCA, feasible and reliable preclinical models are necessary. The purpose of this study was to introduce new techniques to an established preclinical VCA model to accelerate future investigations.
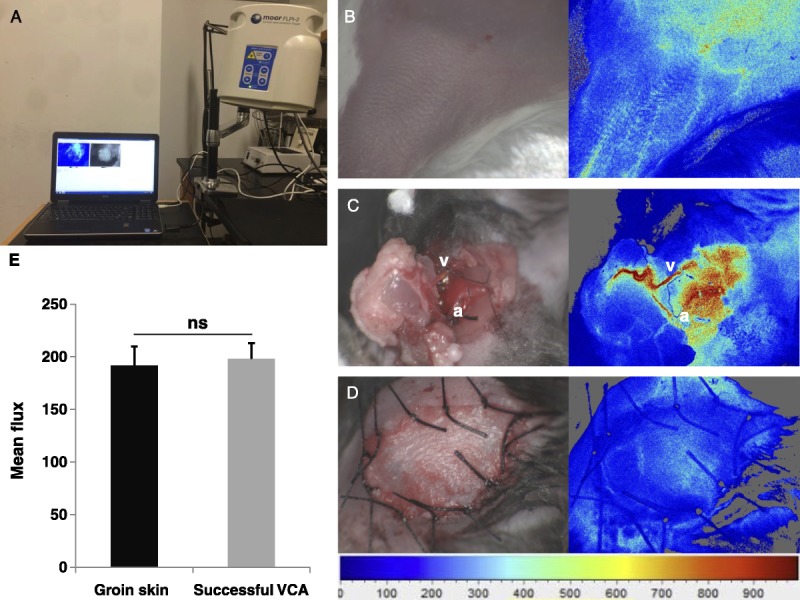
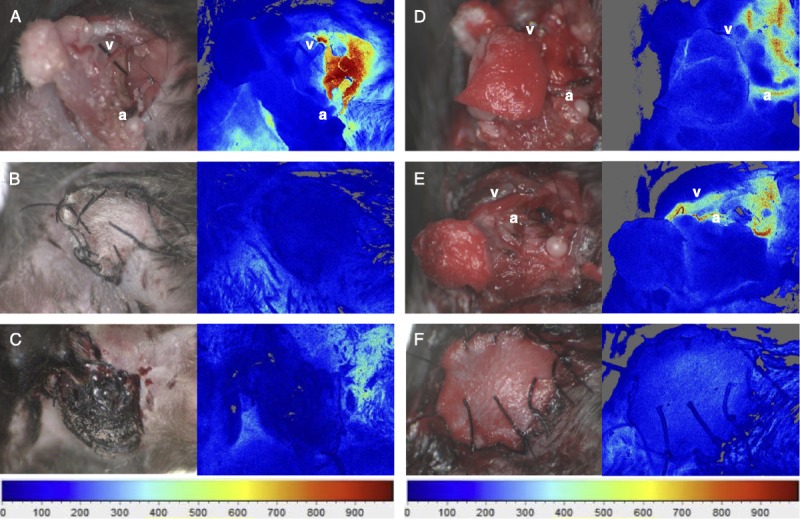
Methods: C57BL/6 (H-2b) and BALB/c (H-2d) mice were used to perform VCA as recipients and donors, respectively. Surgery time, success rate, associated complications, and mortality were analyzed. Blood flow in grafts was interrogated with laser speckle image (LSI).
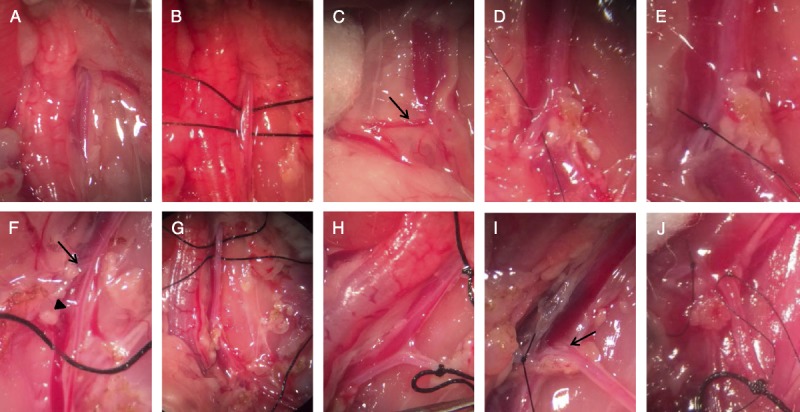
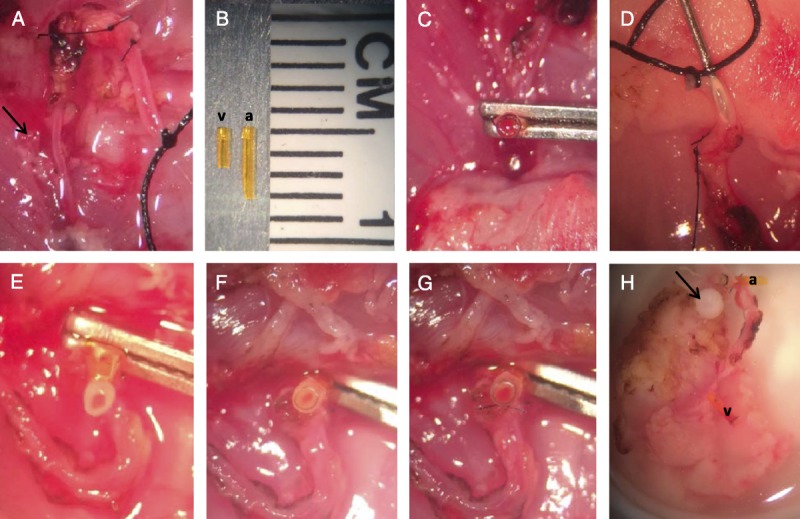
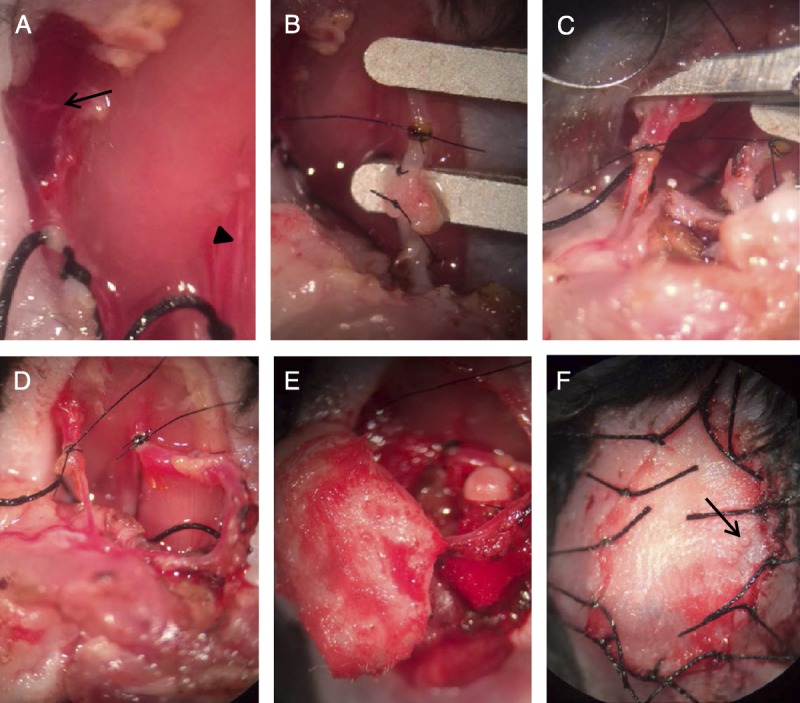
Results: A nonsuture cuff technique was used with the abdominal aorta for end-to-end anastomosis. The cuff technique demonstrated efficiency for donor surgery (52 ± 10 minutes for donor vs. 45 ± 8 minutes for recipient surgery). Successful revascularization was achieved in 27 (90%) of 30 transplants. The majority of surgical complications occurred within 48 hours including artery occlusion, venous occlusion, cerebral stroke, and minor bleeding without mortality. LSI was useful in detecting intraoperative vascular complications with display patterns predictive of complication type.
Conclusions: The described techniques may facilitate a more efficient heterotopic hind limb transplantation mouse model of VCA.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Depletion of donor dendritic cells ameliorates immunogenicity of both skin and hind limb transplants.Front Immunol. 2024 May 10;15:1395945. doi: 10.3389/fimmu.2024.1395945. eCollection 2024. Front Immunol. 2024. PMID: 38799435 Free PMC article.
-
Mouse hind limb transplantation: a new composite tissue allotransplantation model using nonsuture supermicrosurgery.Transplantation. 2010 Dec 27;90(12):1374-80. doi: 10.1097/TP.0b013e3181ff4fc3. Transplantation. 2010. PMID: 21076369
-
A modified heterotopic swine hind limb transplant model for translational vascularized composite allotransplantation (VCA) research.J Vis Exp. 2013 Oct 14;(80):50475. doi: 10.3791/50475. J Vis Exp. 2013. PMID: 24145603 Free PMC article.
-
Cellular activation pathways and interaction networks in vascularized composite allotransplantation.Front Immunol. 2023 May 17;14:1179355. doi: 10.3389/fimmu.2023.1179355. eCollection 2023. Front Immunol. 2023. PMID: 37266446 Free PMC article. Review.
-
Surgical Techniques for Revascularization in Abdominal Wall Transplantation.J Reconstr Microsurg. 2020 Sep;36(7):522-527. doi: 10.1055/s-0040-1709481. Epub 2020 Apr 25. J Reconstr Microsurg. 2020. PMID: 32334436 Review.
Cited by
-
Evolution of the rat hind limb transplant as an experimental model of vascularized composite allotransplantation: Approaches and advantages.SAGE Open Med. 2020 Oct 30;8:2050312120968721. doi: 10.1177/2050312120968721. eCollection 2020. SAGE Open Med. 2020. PMID: 33194200 Free PMC article.
-
Efficacy of single-agent immunosuppressive regimens in a murine model of vascularized composite allotransplantation.Transpl Int. 2020 Aug;33(8):948-957. doi: 10.1111/tri.13618. Epub 2020 May 12. Transpl Int. 2020. PMID: 32299127 Free PMC article.
-
Novel Osteomyocutaneous Flap Model for Vascularized Composite Allotransplantation.JPRAS Open. 2024 Jun 12;41:244-251. doi: 10.1016/j.jpra.2024.05.016. eCollection 2024 Sep. JPRAS Open. 2024. PMID: 39099676 Free PMC article.
-
Manipulating adrenergic stress receptor signalling to enhance immunosuppression and prolong survival of vascularized composite tissue transplants.Clin Transl Med. 2022 Aug;12(8):e996. doi: 10.1002/ctm2.996. Clin Transl Med. 2022. PMID: 35994413 Free PMC article.
-
From Lab to Limb: Unraveling Translational Insights and Significance of Animal Models in Lower Extremity Transplantation.JPRAS Open. 2024 Nov 28;43:232-244. doi: 10.1016/j.jpra.2024.11.018. eCollection 2025 Mar. JPRAS Open. 2024. PMID: 39811586 Free PMC article. Review.
References
-
- Devauchelle B, Badet L, Lengele B, et al. First human face allograft: early report. Lancet. 2006;368:203–209. - PubMed
-
- Dubernard JM, Owen ER, Lanzetta M, et al. What is happening with hand transplants. Lancet. 2001;357:1711–1712. - PubMed
-
- Gilbert R. Transplant is successful with a cadaver forearm. Med Trib Med News. 1964:20–23.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
