

Prognostic value of pathological lymph node status and primary tumour regression grading following neoadjuvant chemotherapy - results from the MRC OE02 oesophageal cancer trial
- PMID: 29465751
- PMCID: PMC5969086
- DOI: 10.1111/his.13491
Prognostic value of pathological lymph node status and primary tumour regression grading following neoadjuvant chemotherapy - results from the MRC OE02 oesophageal cancer trial
Abstract
Aims: Neoadjuvant chemotherapy (NAC) remains an important therapeutic option for advanced oesophageal cancer (OC). Pathological tumour regression grade (TRG) may offer additional information by directing adjuvant treatment and/or follow-up but its clinical value remains unclear. We analysed the prognostic value of TRG and associated pathological factors in OC patients enrolled in the Medical Research Council (MRC) OE02 trial.
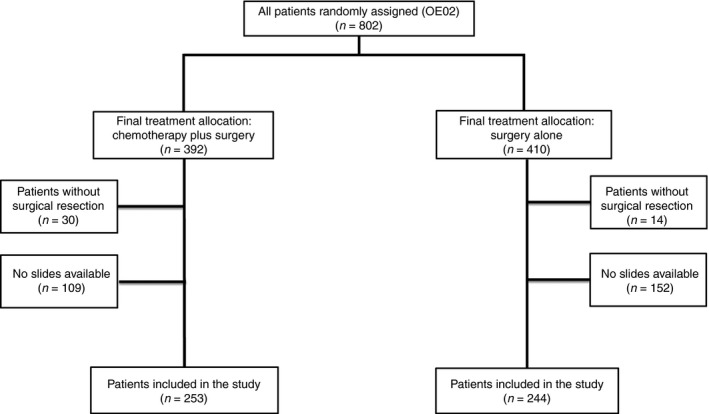
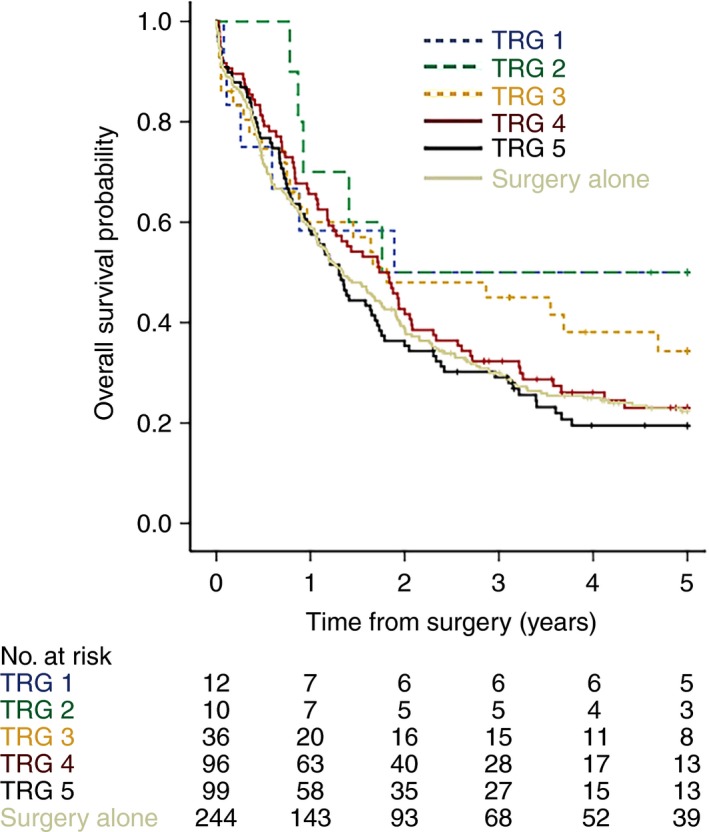
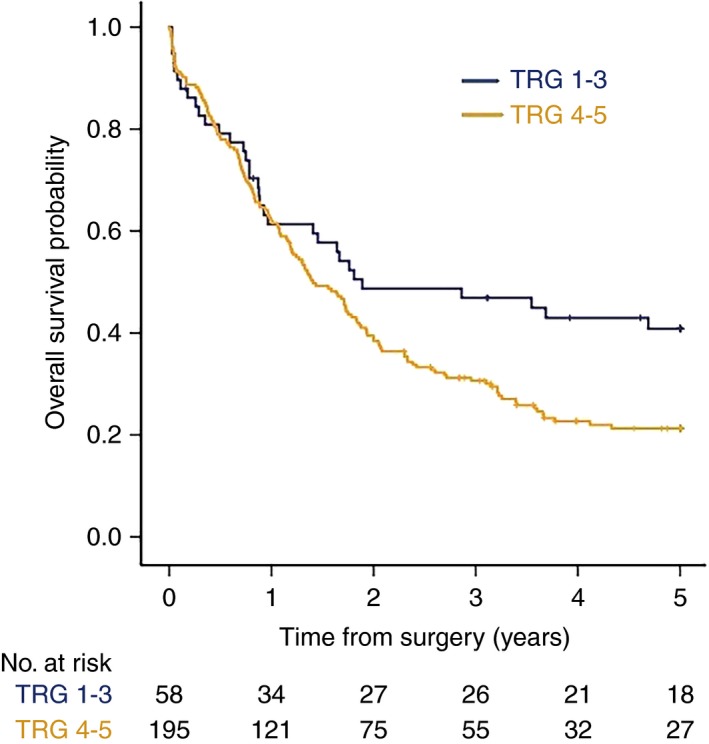
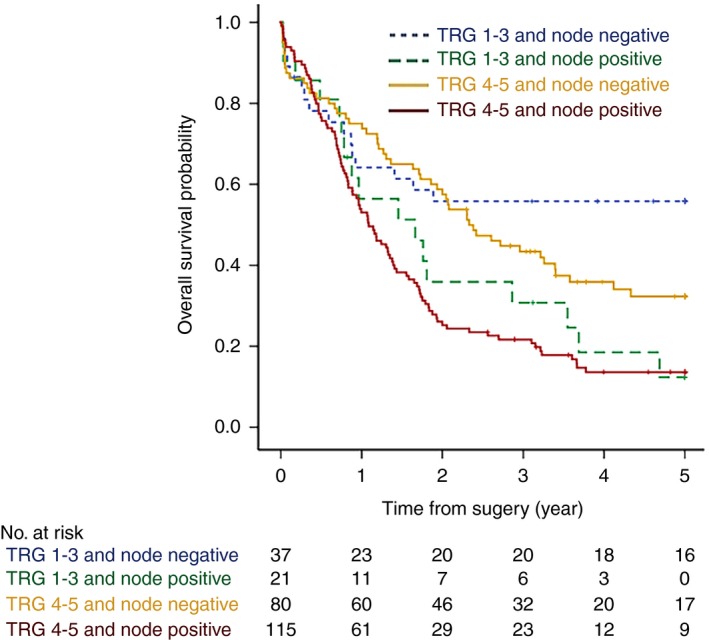
Methods and results: Histopathology was reviewed in 497 resections from OE02 trial participants randomised to surgery (S group; n = 244) or NAC followed by surgery [chemotherapy plus surgery (CS) group; n = 253]. The association between TRG groups [responders (TRG1-3) versus non-responders (TRG4-5)], pathological lymph node (LN) status and overall survival (OS) was analysed. One hundred and ninety-five of 253 (77%) CS patients were classified as 'non-responders', with a significantly higher mortality risk compared to responders [hazard ratio (HR) = 1.53, 95% confidence interval (CI) = 1.05-2.24, P = 0.026]. OS was significantly better in patients without LN metastases irrespective of TRG [non-responders HR = 1.87, 95% CI = 1.33-2.63, P < 0.001 versus responders HR = 2.21, 95% CI = 1.11-4.10, P = 0.024]. In multivariate analyses, LN status was the only independent factor predictive of OS in CS patients (HR = 1.93, 95% CI = 1.42-2.62, P < 0.001). Exploratory subgroup analyses excluding radiotherapy-exposed patients (n = 48) showed similar prognostic outcomes.
Conclusion: Lymph node status post-NAC is the most important prognostic factor in patients with resectable oesophageal cancer, irrespective of TRG. Potential clinical implications, e.g. adjuvant treatment or intensified follow-up, reinforce the importance of LN dissection for staging and prognostication.
Keywords: neoadjuvant chemotherapy; oesophageal carcinoma; tumour regression grade.
© 2018 The Authors. Histopathology published by John Wiley & Sons Ltd.
Figures
References
-
- Allum WH, Stenning SP, Bancewicz J, Clark PI, Langley RE. Long‐term results of a randomized trial of surgery with or without preoperative chemotherapy in esophageal cancer. J. Clin. Oncol. 2009; 27; 5062–5067. - PubMed
-
- van Hagen P, Hulshof MC, van Lanschot JJ et al Preoperative chemoradiotherapy for esophageal or junctional cancer. N. Engl. J. Med. 2012; 366; 2074–2084. - PubMed
-
- Lordick F, Mariette C, Haustermans K, Obermannova R, Arnold D; ESMO Guidelines Committee . Oesophageal cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow‐up. Ann. Oncol. 2016; 27; v50–v57. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
